Thyroid. Hypothyroidism is the result of weight problems. The thyroid gland and its functions
I talked about why it is useful to conduct a regular examination of the thyroid gland using ultrasound. After that, a lot of letters came to the mail with questions about what the norms of the thyroid gland should be.
Therefore, I decided to write a separate article so that everyone can get acquainted with the information.
The thyroid gland is an organ located in the neck, in front, under the larynx. It has the shape of a butterfly and consists of two symmetrical lobes and an isthmus. Since the gland is located directly under the skin, deviations in its structure or structure can be detected even during the initial examination by an endocrinologist by palpation.
The thyroid gland of normal size in most cases is not palpable, except in cases where excessive thinness or the anatomical structure of the patient's neck allows this.
However, with a noticeable increase in the size of the gland during palpation, it is easy to determine:
- the shape of the organ, the size and symmetry of its lobes, the total volume;
- mobility and localization of the gland;
- density and consistency of gland tissue;
- the presence of nodes and volumetric formations.
Unfortunately, the manipulation does not allow to detect formations while maintaining or reducing the normal size of the organ, therefore, the main method for reliable diagnosis of the state of the thyroid gland is ultrasound.
On ultrasound, the thyroid gland is defined as a rounded organ, vaguely resembling a butterfly in shape, with symmetrical lobes and a homogeneous structure.
- The volume of the gland: in women - from 15 to 20 cm3, in men - from 18 to 25 cm3.
- Dimensions of the lobes of the gland: length - 2.5-6 cm, width - 1.0-1.8 cm, thickness - 1.5-2.0 cm.
- Isthmus thickness: 4 to 8 mm.
- Parathyroid glands with a diameter of 2–8 mm, from 2 to 8 units.
In different medical sources of the border normal indicators the size of the lobes and the volume of the organ differ. Studies among the population have shown that the average values of the norm are relative - for example, the population of regions with a constant iodine deficiency is characterized by a general change in the size of the thyroid gland upwards, and this is not a pathology.
Often there is an asymmetry of the organ - the right lobe is usually larger than the left, but it happens vice versa - as idiosyncrasy organism. There have been cases where healthy people one of the lobes was underdeveloped or completely absent.
The difference in the volume of the thyroid gland in men and women is not associated with gender, but with the difference in the physical and physiological parameters of the body.
Normal thyroid size
Although during the menstrual cycle in women there are some fluctuations in the data of ultrasound of the thyroid gland, nevertheless, specialists during the examination take into account, first of all, the age and weight of the patient. In adults, the normal size of the thyroid gland can vary within:
- weight up to 40 kg - up to 12.3 cm3;
- 41–50 kg - up to 15.5 cm3;
- 51–60 kg - up to 18.7 cm3;
- 61–70 kg - up to 22 cm3;
- 71–80 kg - up to 25 cm3;
- 81–90 kg - up to 28.4 cm3;
- 91–100 kg - up to 32 cm3;
- 101–110 kg - up to 35 cm3.
As the data of the list show, the concept of the norm in a healthy person is very relative and often goes beyond the average indicators. In addition, it is allowed to exceed these norms by 1 cm3 or more, provided that the function of the thyroid gland is not impaired.
There are cases of individual underdevelopment (hypoplasia) of the organ with the preservation of its full functionality.
In about 1/6 of the population, the thyroid gland has a pyramidal lobe - an additional structural unit with a base in the middle of the isthmus - which is also one of the variants of the individual norm. Specialists of diagnostic rooms periodically observe the absence of an isthmus between the lobes of the organ in some patients.
To identify pathological changes, a comprehensive analysis of the data of ultrasound examination of the thyroid gland is necessary:
- Contours of the gland - healthy organ has clear, even contours, the change of which indicates the development of the inflammatory process.
- Structure - homogeneous glandular tissue is an indicator of the norm and has a characteristic granularity. With the development of immune inflammatory diseases - autoimmune thyroiditis, diffuse toxic goiter - the structure becomes heterogeneous. Sometimes the heterogeneous structure of the glandular tissue is also found in healthy people of older age groups with increased production of antibodies to certain enzymes of thyroid cells.
- Echogenicity is a certain value of the general acoustic response characteristic of the tissue under study. Echogenicity should be normal, i.e. meet the standards for that body. If echogenicity is reduced, the doctor may suspect the development of an inflammatory process. An increase in echogenicity may indicate acute inflammation or the development of pathological changes.
- Foci of changes are areas characterized by a decrease (hypoechogenicity), absence (anechoicity) or an increase (hyperechogenicity) of the acoustic response of ultrasound. Such formations should not normally be, although the presence of small, up to 4 mm, anechoic areas is allowed - single enlarged follicles of the glandular tissue. Pathological foci, identified in the structure of the tissue, are nodes of the thyroid gland. Nodes can be single or multiple. Solitary small nodules (1-3 mm) are usually not treatable and often disappear on their own over time. Formations larger than 3 mm, as a rule, require clarification of the diagnosis.
- The state of the lymph nodes - the latter should have clear, even contours, no cysts and a normal size (not enlarged).
What does a thyroid ultrasound show?
colloid nodes- formations, which are overgrown follicles. These are benign lesions that almost never degenerate into malignant tumors.
Adenoma A benign tumor that needs to be surgically removed. The presence of a fibrous capsule allows it to be differentiated from other pathologies. It develops with age, mainly in women.
Cyst- fluid-filled formation. Usually observable.
thyroid cancer- a dangerous single node that does not have clear boundaries and a shell. Is different rapid growth, is subject to immediate removal along with the lymph nodes.
When a neoplasm is detected, the patient undergoes additional research- Dopplerography or elastography, to assess changes in the intensity of blood flow in the vessels of an organ, and the cellular and tissue structure of existing formations. If necessary, carried out needle biopsy for histological analysis under ultrasound supervision.
Diffuse toxic goiter- a disease manifested by an increase in the volume of the gland and the heterogeneity of its structure due to the formation of multiple nodes.
Inflammatory diseases (thyroiditis)- distinguish between acute and subacute thyroiditis of infectious and viral origin, arising as complications after tonsillitis, bronchitis, pneumonia, SARS; fibrous thyroiditis - inflammation of the tissue as a result of the abundant growth of its fibrous component; autoimmune chronic thyroiditis - a feature of the body to perceive thyroid cells as foreign, resulting in an inflammatory process.
Goiter of the thyroid gland- an increase in volume due to tissue growth. Euthyroid goiter does not affect the function of the organ, hypo- and hyperthyroid goiters are associated with corresponding dysfunctions. Perhaps the development of endemic goiter among the population of areas with a low content of iodine in the environment, as well as some hypertrophy of the thyroid gland during pregnancy.
Hypoplasia of the thyroid gland- congenital underdevelopment of the organ due to endocrine disorders during pregnancy of the mother or insufficient intake of iodine in the body.
Thyroid atrophy- a decrease in its size as a result of the gradual replacement of the glandular tissue with connective tissue, combined with the development of hypothyroidism, requiring constant replacement therapy.
Thus, when making an accurate diagnosis by an endocrinologist, the results of ultrasound examination (ultrasound) are analyzed in combination with other indicators of the patient's health. The set of complaints individual symptoms, general well-being, blood tests and functional diagnostic data allows the doctor to determine the individual boundaries of the norm and pathology and choose the best means of treating the patient.
Dear readers, if you have any questions, then ask them in the comments, I will try to answer them in detail.
Introduction
thyroid gland, gland internal secretion, similar in shape to a butterfly, is a unique organ.
Ancient philosophers associated it with fire, thereby emphasizing its significance for the body. Very small in size, no more than 18 ml in women and 25 ml in men, it is involved in almost all life processes. Without it, the functioning of the human body is impossible. Growth and development, metabolic processes, respiration, digestion... Thyroid dysfunction creates many problems in the work of all body systems.
In recent years, the number of people with identified disorders in the thyroid gland has sharply increased: diffuse and nodular goiter, Graves' disease, autoimmune thyroiditis, oncological diseases. There are enough reasons for disappointing statistics: environmental degradation, reduced immune defense of the human body, lack of iodine, lack of planned medical prevention, unbalanced nutrition, stress as a provoking factor. Currently, thyroid diseases are leaders in the list of diseases of the endocrine system.
Quite a lot has been written about the treatment and prevention of thyroid diseases; on the Internet, you can find tips and tricks to combat the disease. However, it should be remembered that the treatment, selection and prescription of drugs should be handled by a specialist - an endocrinologist. And before you start using any method of treatment, you need to consult a doctor.
In this book, we will talk about the structural features of the thyroid gland, its functions, diseases of this vital organ, as well as give useful advice and talk about methods for examining and treating thyroid diseases.
Chapter 1 Thyroid Gland
"Butterfly" flies on iodine, without it it does not fly!
The thyroid gland and its functions
The thyroid gland is a gland of the endocrine system that stores iodine and produces iodine-containing hormones: thyroxine and triiodothyronine, which are involved in the regulation of metabolism and the growth of individual cells, as well as the body as a whole.
The gland, along with other organs of the endocrine system, performs its main function: it maintains the constancy of the internal environment of the body, which is necessary for its normal functioning.
The thyroid gland is located under the thyroid cartilage and has the shape of a butterfly (see Fig. 1).
Rice. 1. The shape of the thyroid gland can be compared with the letter "H" or with a butterfly
Interesting fact:
A brief morphological description of the thyroid gland as early as the 2nd century BC. BC e. given by Galen. He considered it part of the vocal apparatus.
Continued the study of the thyroid gland Vesalius.
And the name of this organ was given by Barton in 1656. He proceeded from its shape and purpose: it, like a shield, protects the organs located on the neck.
The concept of the function of internal secretion, which is carried out by the thyroid gland, was formulated by King.
Karling later described cretinism in people without a thyroid gland.
The gland consists of two lobes and an isthmus. The isthmus is a part of the thyroid tissue that connects the right and left lobes. It is located at the level of the second or third tracheal ring.
The lateral lobes surround the trachea and are attached to it by connective tissue.
An additional, pyramidal lobe may depart from the isthmus or one of the lobes. It is a long process that reaches the upper part of the thyroid cartilage or hyoid bone.
The additional proportion is not considered a deviation, rather it is an individual feature of the organism (see Fig. 2).
The thyroid gland is located in the middle third of the neck. Run your hand over the neck and you will find dense cartilage that shifts when you swallow. This is the thyroid cartilage. In men, it is larger than in women, and is called the Adam's apple.

Rice. 2. The lower parts of the thyroid gland are short and wide, while the upper ones are high, narrow and slightly divergent.
The thyroid cartilage somewhat covers the thyroid gland, its upper pole reaches it. It got its name from its functions: it serves as a shield, covers important organs lying on the neck.
The main characteristics of the gland: weight, height and width of shares, volume.
The thyroid gland of an adult human weighs on average 20–40 g, while in a newborn it is only 2–3 g.
Normally, the height and width of the lobes of the thyroid gland are 3–4 and 1–2 cm, respectively, and the width is 7–11 cm.
In order to understand whether the thyroid gland is enlarged, the doctor palpates (probes) it and compares the size of each lobe with the size of the terminal nail phalanx of the thumb on the patient's hand. Normally, their sizes should be the same.
Look at your fingers and you'll see how big your thyroid should be (see Figure 3).

Rice. 3. Nail phalanx of the thumb
The World Health Organization (WHO) distinguishes three degrees of thyroid size, which the doctor evaluates during examination and palpation (table 1).
Table 1
Degrees of thyroid size

If a goiter is detected, you should understand what the volume of the thyroid gland is. This is important for further treatment planning and follow-up.
Volume is the main indicator of the size of the thyroid gland.
Normally, it is up to 18 ml in women and up to 25 ml in men.
The volume of the thyroid gland is calculated using a special formula during an ultrasound examination (ultrasound).
The thyroid gland is made up of follicles. Follicles are communities of thyrocytes (thyroid cells), these are closed hollow formations of various shapes. Their walls are formed by cells that produce colloid - a thick yellowish mucous liquid.
The smallest follicles have a diameter of 0.03 to 0.1 mm, and their average size is 0.15 mm. The largest follicles can be seen with the naked eye on a transverse section of the thyroid gland.
Thyroid hormones
The thyroid gland is an endocrine gland. Its main function is the production of hormones, which include iodine, without which the normal functioning of the body is impossible (Fig. 4).
Thyroid hormones control metabolism, the processes of maturation of tissues and organs, and activate mental activity. They are necessary for active growth, the formation of bones of the skeleton, in women - for the development of the mammary glands.
The term "hormone" in Greek - "I excite", "I encourage". It was introduced into medical practice by Bayliss and Starling. Thyroxin was discovered by the American E. Kendall in 1914, and in 1927 C. Harrington synthesized it for the first time. Decreased production of thyroid hormones in childhood body growth stops. In this case, you should immediately consult a doctor!
As already mentioned, the thyroid gland produces thyroid hormones: thyroxine and triiodothyronine.
In another way, thyroxine is called T4, as it carries four iodine atoms. In the blood and tissues of the human body, the T4 hormone is converted into the T3 hormone - triiodothyronine, which carries three iodine atoms.
Initially, the thyroid gland produces 70% T4 and 30% T3, but the main amount of T3 is formed during the breakdown of T4 in the body.
The biological effect of hormones is realized as follows: the hormone attaches to the receptor and, connecting with it, triggers a series of reactions already in the cell of the organ.
Since thyroid hormones are responsible for the development of the body, proper metabolism and energy, receptors are everywhere: in the brain and in all tissues of the human body.
The functions of thyroid hormones are as follows:
Increase the intensity of oxidative reactions in cells;

Rice. 4. The main function of the thyroid gland is the production of hormones, without which the normal functioning of the body is impossible.
Influence the processes occurring in mitochondria, the cell membrane;
Maintain hormonal excitability of the main nerve centers;
Participate in normal functioning heart muscle;
Ensure the functioning of the immune system: stimulate the formation of T-lymphocytes responsible for fighting infection.
The thyroid gland is actively supplied with blood, it has a lot of blood vessels.
Active blood supply is carried out by four main arteries. The two superior thyroid arteries arise from
external carotid, and the two lower ones - from the thyroid cervical subclavian arteries.
The outflow of blood from the gland occurs through paired veins. It is 4-6 ml / min / g and slightly exceeds the blood flow in the kidneys and brain.
Previously, active blood supply to the thyroid gland created difficulties during surgery on this organ. Surgeon Theodor Kocher developed safe approaches to thyroid surgery, for which he received Nobel Prize. And it was the knowledge of the characteristics of the blood supply to the thyroid gland that helped him develop a certain tactic of surgical intervention.
The thymus gland (thymus or thymus gland) is an organ of human immunity and hematopoiesis, responsible for the synthesis of certain types of white blood cells. The gland is located directly behind the sternum in the superior mediastinum. Rarely, an atypical location of thymus lobules in the thickness of the thyroid gland, in fatty tissue posterior mediastinum or between the muscles of the neck. This arrangement is called aberrant and occurs in a quarter of the world's population. A predisposing factor for the aberrant location of the thymus gland is congenital heart defects.
The organ has a pinkish-gray color and a soft texture with a lobed structure. A healthy thymus consists of two large lobes and is shaped like a fork with two teeth, which gave rise to the second name of the organ. A damaged gland can change its shape. From above, the lobes are covered with a connective tissue capsule with bridges extending into the thickness of the gland. The bridges divide the lobes into smaller lobes. The mass of the gland in a newborn and infant is about 15-17 g, the size does not exceed 4-5 cm, and the thickness is 0.5 cm. The thymus reaches its maximum size by the onset of puberty - 8-16 cm in length, and the mass increases by two times. After that, in adults, the gland gradually undergoes a reverse development - involution - and practically merges with the fatty tissue surrounding it. Involution can be physiological (age-related) and accidental - under stressful effects on the body.
The thymus is supplied by branches of the internal thoracic artery, aorta, and thyroid arteries. outflow blood is coming along the internal thoracic and brachiocephalic veins. It is innervated by branches of the vagus nerves and the sympathetic trunk.
Histology of the thymus
The thymus develops from the ectoderm and contains cells of epithelial and hematopoietic origin. Conventionally, the entire substance of the thymus gland is divided into cortical and cerebral. The cortex contains:
- cells that form the hemato-thymic barrier - supporting cells;
- stellate cells that secrete hormones;
- “nanny” cells, between the processes of which T-lymphocytes develop and mature;
- T-lymphocytes - white blood cells;
- thymic macrophages.
The medulla contains a large number of maturing T-lymphocytes. When these cells go through all the stages of their development, they are sent into the bloodstream through venules and veins, ready to carry out immune function.
Thus, the T-lymphocyte appears and begins to mature in the cortical substance, and then, as it matures, it passes into the medulla. This process lasts about 20-22 days.
As they move from the cortex to the medulla and from the medulla to the general circulation, T-lymphocytes undergo selection - positive and negative selection. In the course of it, the cells "learn" to recognize the alien and distinguish their own from the alien. According to scientists, only 3-5% of T cells pass both stages of selection and enter the systemic circulation. Selection allows you to determine which of the cells fully perform their function, and which do not need to be released into the bloodstream.
What processes are regulated by the thymus?
The main role of the thymus is in the differentiation and maturation of cells T cell immunity- T-lymphocytes. Proper development and selection of these cells leads to the formation of many receptors for foreign substances and, as a result, to an immune response upon contact with them.
The second function of the thymus gland is the synthesis of hormones, such as:
- thymosin;
- thymulin;
- thymopoietin;
- insulin-like growth factor-1;
- thymic humoral factor.
Thymus hormones affect the function of T-lymphocytes and the degree of their activity. A number of studies have shown an activating effect of thymic hormones on the central nervous system.
thymosin
This hormone is a polypeptide protein synthesized in the epithelial cells of the organ stroma and performs the following functions:
- regulation of the development of the musculoskeletal system by controlling calcium metabolism;
- regulation of carbohydrate metabolism;
- increased synthesis of pituitary hormones - gonadotropins;
- an increase in the synthesis of T-lymphocytes before puberty;
- regulation of antitumor defense.
With its insufficient activity or secretion, T-cell failure develops in the human body - up to the absolute absence of cells. Clinically, this is manifested by a sharp decrease in protection against infections, the dominance of severe and atypical forms infectious diseases.
thymopoietin
Thymopoietin is a 49 amino acid peptide hormone. It is involved in the differentiation and maturation of T cells in the cortex and medulla and determines in which of several types of T lymphocytes a particular cell matures.
Another function of the hormone is to block neuromuscular transmission. It also has the property of immunomodulation - this is the ability of the hormone, if necessary, to suppress or enhance the synthesis and activity of T-cells.
Timulin
The protein hormone thymulin influences the final stages of T-cell differentiation. It stimulates cell maturation and recognition of foreign agents.
From common influences on the body, there is an increase in antiviral and antibacterial protection by increasing the production of interferons and enhancing phagocytosis. Thymulin also accelerates tissue regeneration. The determination of thymulin is decisive in evaluating the effectiveness of the treatment of thymus diseases.
Other hormones
In its own way chemical structure insulin-like growth factor-1 is similar to insulin. Regulates the mechanisms of differentiation, development and growth of cells, participates in glucose metabolism. In muscle cells, the hormone has growth-stimulating activity, is able to shift metabolism and promote increased fat burning.
Thymus humoral factor is responsible in the body for stimulating the reproduction of lymphocytes.
Thymus gland diseases
Diseases of the thymus practically do not occur in adults, most often the pathology is recorded in children under the age of one year. The most common and most studied diseases of the thymus are:
- MEDAC syndrome;
- DiGeorge syndrome;
- myasthenia gravis;
- various tumors.
Inflammation of the thymic stroma is rare.
Tumors of the thymus gland include the following:
- thymomas and hyperplasia - benign neoplasms in which the gland is enlarged in size;
- hypoplasia, or underdevelopment of the organ;
- T-cell lymphoma;
- pre-T-lymphoblastic tumors with transformation into leukemia or cancer;
- neuroendocrine tumors.
Thymus diseases have a variety of clinical manifestations, but some symptoms are common to all:
- respiratory failure;
- heaviness of the eyelids;
- chronic fatigue;
- muscle weakness and rarely muscle pain;
- decreased resistance to infections.
Most of the diseases of the thymus are dangerous for the life of the child, therefore, if a pathology of the thymus gland is suspected, urgent consultations of an immunologist and a hematologist are necessary.
The doctor's examination plan includes:
- general and biochemical analyzes blood;
- determination of the activity of thymus hormones;
- immunogram;
- Ultrasound of the gland.
What is a colloidal thyroid nodule?
Colloidal nodule of the thyroid gland, what is it? This is a pathology characterized by the appearance benign neoplasms. Their presence is not dangerous for human life, but plays an important role in the diagnosis of diseases of the endocrine system. Colloidal nodes in the thyroid gland are found in most patients of endocrinologists, but most often they are benign. A colloid is a viscous mass that fills the follicle of the gland, so it is not considered atypical for this body. Such a substance is formed in the tissues responsible for the production of thyroid hormones. Microscopic analysis reveals that the node consists of glandular cells, blood and colloid. It does not contain foreign inclusions, which means it is safe for health.
Reasons for the development of the disease
The role of the thyroid gland in human body cannot be overestimated. The organ, which is relatively small, must produce many hormones that are distributed throughout the body. Chronic and infectious diseases, stress, unfavorable environmental conditions make the gland work at an accelerated pace, which leads to organic and functional disorders. Some parts of the body begin to produce hormones unevenly, which is accompanied by vasodilation and an increase in tissue density. This is how colloidal nodes of the thyroid gland are formed.
The main reasons for the appearance of colloid nodes in the thyroid gland are: unfavorable environmental conditions, stress, high physical activity, chronic diseases, iodine deficiency in the body, malnutrition, puberty, pregnancy. Iodine deficiency is the most common cause of nodular changes. All residents of our country are deficient in this element, with the exception of people living in the Crimea and the Far East. Iodine is considered the most important substance, without which the thyroid gland cannot produce hormones.
Clinical picture
In the early stages of node development, no symptoms appear. More often the reason for going to the doctor is a significant increase in the size of the gland. In this case, symptoms of the mechanical impact of the node on the surrounding tissues appear: pressure in the area of the organ, difficulty in swallowing and breathing, sore throat, cough. On the late stages the disease changes the timbre and volume of the voice. Constant squeezing of large vessels and nerve endings can affect the central nervous system: headaches, dizziness, tinnitus appear. Pain in the neck area occur when rapid increase node in size, accession of hemorrhages or inflammatory processes.
Depending on the prevalence pathological process the thyroid gland can be enlarged on one or both sides. If the size of the node exceeds 1 cm, a person can detect it on their own. Depending on the degree of dysfunction of the thyroid gland, the clinical picture of the disease may vary. Symptoms of hypothyroidism appear when the colloidal mass begins to replace healthy cells glands. General weakness appears, intellectual abilities decrease, appetite is lost. The patient's body swells, metabolic processes in the body slow down, weight begins to grow, the skin becomes dry.
When the thyroid gland begins to produce an increased amount of hormones, a person experiences symptoms of hyperthyroidism. This condition manifests itself in the form of irritability, fatigue, aggression. Appetite increases, but the person loses weight, digestive processes are disturbed, which manifests itself in the form of diarrhea. Body temperature may rise and tachycardia develop. If the process of hormone production is not disturbed, the only sign of the disease will be the compaction of the thyroid gland and its increase in size. Growing nodes compress large vessels and nerve endings, which leads to a feeling of a lump in the throat, problems with breathing and swallowing.
Diagnosis and treatment of the disease
It is possible to determine the nature of the nodes in the thyroid gland only after complete examination. It begins with palpation of the cervical region, in which pathological changes are detected. Additional diagnostic methods include: biopsy, ultrasound of the thyroid gland, CT or MRI, blood test for hormones, radioisotope scanning. Based on results diagnostic procedures the endocrinologist reveals the presence of organic and functional changes in the thyroid gland. A biopsy is prescribed in the presence of large colloid nodes. Despite the fact that in most cases nodal changes are benign, it is necessary to study the structure of the largest of them.

With an asymptomatic course of the pathological process, treatment may not begin immediately. Neoplasm is recommended to be observed for several years. The doctor may prescribe iodine preparations to restore thyroid function. The patient may wish to get rid of the colloid node surgically, but doctors do not recommend such operations. After resection, the thyroid tissue begins to grow faster.
Surgery should be performed if there is absolute readings: squeezing by a knot of large vessels and nerve endings, the production of an increased amount of hormones. Radical operations are also used in the malignant nature of the course of the pathological process. Depending on the size of the tumor and the presence of metastases, the thyroid gland can be partially or completely removed.
In other cases, the treatment of colloid nodes begins with the elimination of the cause of their occurrence. For example, if toxic goiter contributed to the accumulation of colloidal mass, it is necessary to regulate the production of thyroid hormones and restore the functions of all organs and systems. If the cause of the appearance of nodal changes is not clarified, it is carried out symptomatic therapy, aimed at eliminating unpleasant sensations associated with the mechanical impact of the colloid node on the surrounding tissues.
There are several ways conservative treatment: drug therapy aimed at eliminating dysfunction of the thyroid gland; minimally invasive surgical interventions — laser treatment or sclerosis of colloid nodes. Before prescribing a particular drug, a blood test for hormones should be performed to assess functionality organ. The patient should be asked about the presence of allergic reactions to medicines. In most cases, derivatives of thyroxine and thyroidin are prescribed.
Properly selected treatment regimen avoids the development of dangerous complications. Colloidal nodes are a fairly common phenomenon; there are no specific preventive measures. A person should carefully monitor their health, regularly visit an endocrinologist, eat right and take iodine preparations. It is necessary to avoid exposure to radiation and visiting places with unfavorable environmental conditions. This will help maintain the health of the thyroid gland, normalize the structure of its tissues, improve general state organism.
Hormonal functions of the thyroid gland and their disorders
Location
Associating deviations from the norm in their condition with the pathology of the thyroid gland, patients are wondering where the thyroid gland is located, since the diagnosis begins with this - with palpation.

The gland is located under the larynx, at the level of the fifth or sixth cervical vertebra. It covers the top of the trachea with its lobes, and the isthmus of the gland falls directly into the middle of the trachea.
The shape of the gland resembles a butterfly with wings tapering upwards. The location does not depend on gender, in a third of cases there may be an insignificant additional part of the gland in the form of a pyramid, which does not affect its functioning, if present from birth.
In terms of mass, the thyroid gland reaches 25 grams, and in length no more than 4 cm. The average width is 1.5 cm, the same thickness. The volume is measured in milliliters and is up to 25 ml for men and up to 18 ml for women.
Functions
The thyroid gland is an endocrine organ responsible for the production of hormones. The functions of the thyroid gland are hormonal regulation through the production of certain types of hormones. Thyroid hormones include iodine in their composition, since another function of the gland is the storage and biosynthesis of iodine into a more active organic function.

Gland hormones
Patients who are referred for laboratory diagnosis of thyroid diseases mistakenly believe that they are examining thyroid hormones TSH, AT-TPO, T3, T4, calcitonin. It is important to distinguish which hormones are produced by the thyroid gland, and which are other organs of internal secretion, without which the thyroid gland simply will not work.
- TSH is a thyroid-stimulating hormone that is produced by the pituitary gland, not the thyroid gland. But it regulates the work of the thyroid gland, activates the capture of iodine from the blood plasma by the thyroid gland.
- Ab-TPO is an antibody to thyroperoxidase, a non-hormonal substance produced by immune system as a result of pathological processes and autoimmune diseases.
Directly thyroid hormones and their functions:
- Thyroxine - T4 or tetraiodothyronine. Represents thyroid hormones, is responsible for lipid metabolism, lowering the concentration of triglycerides and cholesterol in the blood, supports bone tissue metabolism.
- Triiodothyronine - T3, the main thyroid hormone, since thyroxine also tends to be converted to triiodothyronine by attaching another iodine molecule. Responsible for the synthesis of vitamin A, lowering the concentration of cholesterol, activating metabolism, accelerating peptide metabolism, normalizing cardiac activity.
- Thyrocalcitonin is not a specific hormone, since it can also be produced by the thymus and parathyroid glands. Responsible for the accumulation and distribution of calcium in bone tissue essentially reinforcing it.

Based on this, the only thing the thyroid gland is responsible for is the synthesis and secretion of thyroid hormones. But the hormones produced by it perform a number of functions.
secretion process
The work of the thyroid gland does not even begin in the gland itself. The process of production and secretion, first of all, begins with the "commands" of the brain about the lack of thyroid hormones, and the thyroid gland implements them. The secretion algorithm can be described in the following steps:
- First, the pituitary and hypothalamus receive a signal from the receptors that the blood levels of thyroxine and triiodothyronine are low.
- The pituitary gland produces TSH, which activates the uptake of iodine by thyroid cells.
- Iron, capturing the inorganic form of iodine obtained from food, begins its biosynthesis into a more active, organic form.
- Synthesis occurs in the follicles that make up the body of the thyroid gland, and which are filled with a colloidal fluid containing thyroglobulin and peroxidase for synthesis.
- The resulting organic form of iodine is attached to thyroglobulin and released into the blood. Depending on the number of attached iodine molecules, thyroxin is formed - four iodine molecules, or triiodothyronine - three molecules.
- In the blood, T4 or T3 is released separately from globulin, and it is again captured by gland cells for use in further synthesis.
- Pituitary gland receptors receive a signal about enough hormones, the production of TSH becomes less active.
Accordingly, having detected signs of thyroid disease, the doctor prescribes a study not only of the concentration of thyroid hormones, but also of the hormones that regulate it, as well as antibodies to an important component of the colloid - peroxidase.
gland activity
At the moment, medicine divides all pathologies of the thyroid gland into three conditions:
- Hyperthyroidism is a dysfunction of the thyroid gland, in which secretion activity increases and an excess amount of thyroid hormones enters the blood, metabolic processes in the body increase. Thyrotoxicosis is also included in the disease.
- Hypothyroidism is a dysfunction of the thyroid gland, in which an insufficient amount of hormones is produced, as a result of which metabolic processes slow down due to lack of energy.
- Euthyroidism - diseases of the gland, as an organ, which do not have any hormonal manifestations, but are accompanied by pathology of the organ itself. Among the diseases, this includes hyperplasia, goiter, nodular formations.

Diseases of the thyroid gland in women and men are diagnosed through the TSH index, a decrease or increase in which indicates the reactivity or hypoactivity of the gland.
Diseases
In women, symptoms of thyroid disease appear more often, since hormonal fluctuations are reflected in the menstrual cycle, which makes the patient seek medical help. Men cheat more often typical symptoms thyroid glands for fatigue and overexertion.
The main and most common diseases:
- Hypothyroidism;
- Nodular, diffuse or mixed goiter;
- Malignant tumors of the gland.

Each of these diseases is characterized by a special clinical picture and stages of development.
Hypothyroidism
This is a syndrome of chronic decrease in the secretion of T3 and T4, which helps to slow down the body's metabolic processes. At the same time, the symptoms of thyroid disease may not make themselves felt for a long time, progress slowly, and disguise themselves as other diseases.
Hypothyroidism can be:
- Primary - at pathological changes in the thyroid gland;
- Secondary - with changes in the pituitary gland;
- Tertiary - with changes in the hypothalamus.
The causes of the disease are:
- Thyroiditis, which occurs after inflammation of the thyroid gland;
- iodine deficiency syndrome;
- Rehabilitation after radiation therapy;
- Postoperative period of removal of tumors, goiters.

Hypofunctional thyroid disease symptoms are as follows:
- slowdown heart rate, heart rate;
- dizziness;
- pale skin;
- Chills, trembling;
- Hair loss, including eyebrows;
- Swelling of the face, legs, hands;
- Voice changes, its roughness;
- constipation;
- An increase in the size of the liver;
- Weight gain despite decreased appetite;
- Loss of strength, emotional inertia.
Hypothyroidism is usually treated hormonal drugs replenishing the lack of thyroid hormones in the body. But it should be understood that such treatment is advisable in a chronic case, which is diagnosed most often. If the disease is detected in the early stages, there is a chance to stimulate the work of the body by eliminating the root causes and temporarily taking another class of hormones.

This disease is called the lady's disease, since there are nine women for ten patients diagnosed with hyperthyroidism. Excessive production of hormones leads to an acceleration of metabolic processes, excitation of cardiac activity, disturbances in the work of the central nervous system and ANS. Pronounced signs of the disease and the advanced form is called thyrotoxicosis.
Reasons for the development of pathology:
- Graves', Plummer's syndrome - goiters of an autoimmune or viral nature;
- Malignant tumors in the thyroid gland or pituitary gland;
- It may develop as a result of long-term treatment with arrhythmic drugs.
Often, the disease overtakes women after the onset of menopause due to hormonal imbalance, not being a consequence of tumors or goiters.
In this case, the main signs of thyroid gland in women:
- accelerated heartbeat;
- Atrial fibrillation;
- Humidity, hotness of the skin;
- Trembling of the fingers;
- Tremor can reach amplitudes, as in Parkinson's disease;
- Increased body temperature, fever;
- increased sweating;
- Diarrhea with increased appetite;
- Decrease in body weight;
- An increase in the size of the liver;
- Irritability, irascibility, insomnia, anxiety.

Treatment involves taking thyreostatics - drugs that reduce the activity of the secretion of thyroid hormones. Thyreostatics include drugs Thiamazole, Diiodothyrosine, as well as drugs that prevent the absorption of iodine.
In addition, a special diet is prescribed, in which alcohol, coffee, chocolate, hot spices and spices that can excite the central nervous system are excluded. Additionally, adrenergic blockers are prescribed to protect the heart muscle from harmful effects.
The disease has vivid symptoms - already from the second stage of goiter, the gland increases, which means that the entire neck area above the collarbone, where the thyroid gland is located, acquires distorted outlines.
Goiter can be nodular, diffuse and diffuse-nodular. The causes of the disease are sufficiently differentiated - it may be a lack of iodine, on its own developing syndrome and excess hormones.
Symptoms depend on the degree of goiter, of which there are five in medicine:
- In the first degree, the isthmus of the gland increases, which can be felt when swallowing;
- The second degree is characterized by an increase in both the isthmus and the lateral lobes of the gland, which are visible when swallowing and are well felt on palpation;
- At the third stage, the gland covers the entire wall of the neck, distorting its outlines, visible to the naked eye;
- The fourth degree is characterized by a clearly visible goiter, even visually, by a change in the shape of the neck;
- The fifth degree is indicated by a huge goiter, which compresses the trachea, blood vessels and nerve endings of the neck, causes coughing, difficulty breathing, swallowing, tinnitus, memory and sleep disorders.

characteristic, but nonspecific symptom This disease of the thyroid gland in women is a strong protrusion of the eyes, amenorrhea up to six months or more, which is often confused with early menopause.
Treatment consists of hormone therapy in the early stages, in the later stages, surgical intervention is proposed to remove part of the organ.
In addition, treatment depends on the type of goiter, as Graves' syndrome, euthyroid goiter, Plummer's syndrome and Hashimoto's syndrome are subdivided. Accurate determination is possible only with complex diagnostics.
Malignant formations
Develop against the background chronic diseases thyroid glands that did not respond to treatment. The growth of cells in the gland can be provoked and unauthorized.
The prognosis is positive, since in most cases it is diagnosed on early stage and treatable. Vigilance requires only possible relapses.

Symptoms:
- Pain in the neck;
- Seals, the growth dynamics of which is noticeable even within two weeks;
- Hoarse voice;
- breathing difficulties;
- bad swallowing;
- Sweating, weight loss, weakness, poor appetite;
- Cough of non-infectious nature.
With timely diagnosis, it is enough drug therapy. In later stages, surgical removal is indicated.
Diagnostics
Diagnosis of any disease of the thyroid gland begins with the collection of anamnesis. Then an ultrasound is prescribed for:
- Timely detection of nodes, cysts, tumors of the thyroid gland;
- Determining the size of an organ;
- Diagnosis of deviations from the norm in size and volume.

Laboratory diagnostics involves the analysis of:
- AT-TPO;
- T3 - general and free;
- T4 - general and free;
- Tumor markers for suspected tumor;
- General analysis of blood and urine.
In some cases, a biopsy of the tissues of the organ may be prescribed to clarify the diagnosis, if laboratory diagnosis was not enough. It is not recommended to independently interpret the test results and make a diagnosis, since the norm of thyroid hormones is different for each gender, age, disease, and the impact of chronic diseases. Self-treatment autoimmune and especially oncological diseases can end with a threat to health and life.
How safe is thyroid cancer surgery?
 Treatment of thyroid hyperplasia
Treatment of thyroid hyperplasia
What does the appearance of a cough with a thyroid gland mean?
 Flow features autoimmune thyroiditis
Flow features autoimmune thyroiditis
 How to recognize and treat thyroid cysts
How to recognize and treat thyroid cysts
 Reasons for the development of adenoma in the thyroid gland
Reasons for the development of adenoma in the thyroid gland
The thyroid gland consists of two lobes and an isthmus. The lobes are adjacent to the left and right to the trachea, the isthmus is located on the anterior surface of the trachea. Sometimes an additional pyramidal lobe extends from the isthmus or more often the left (rarely the right) lobe of the gland. Normally, the mass of the thyroid gland is from 20 to 60 g, the size of the lobes varies within 5-8´2-4´1-3 cm.
During puberty, the mass of the thyroid gland increases, and decreases in old age. Women have a larger thyroid gland than men; during pregnancy, its physiological increase occurs, which disappears on its own within 6-12 months.
after childbirth.
The thyroid gland has an external and internal connective tissue capsule. Formed by the outer capsule ligamentous apparatus fixing the gland to the trachea and larynx (Fig.). The upper border of the gland (lateral lobes) is the thyroid cartilage, the lower - 5-6 tracheal rings. The isthmus is located at the level of I-III or II-IV cartilages of the trachea.
The thyroid gland is one of the most vascularized organs with a developed arterial and more powerful venous systems. Blood enters the gland through two superior thyroid arteries (branches of the external carotid artery) and two inferior thyroid arteries, which form anastomoses between themselves. The venous and lymphatic systems carry out the outflow from the thyroid gland of blood and lymph containing thyroid hormones, thyroglobulin, and in pathological conditions, antithyroid antibodies, thyroid-stimulating and thyroblocking immunoglobulins.
The innervation of the thyroid gland is carried out by branches of both the vagus nerve (parasympathetic) and branches of the cervical ganglia (sympathetic).
The main structural and functional unit of the thyroid gland are follicles - vesicles of various shapes, often rounded, with a diameter of 25-500 microns, separated from each other by thin layers of loose connective tissue with large quantity blood and lymph capillaries.
Their lumen is filled with a colloid - a structureless mass containing thyroglobulin, which is synthesized by follicular, or the so-called A-cells that form the wall of the follicle. These are epithelial cells of a cubic or cylindrical (with an increase in functional activity) shape. With a decrease in thyroid function, they flatten. Along with the follicles in the thyroid gland, there are interfollicular islands of epithelial cells (B cells, Ascanazi cells), which are the source of the formation of new follicles.
Ascanazi cells are larger than A-cells, have a zosinophilic cytoplasm and a rounded centrally located nucleus: biogenic amines, incl. serotonin. In addition to A- and B-cells, the thyroid gland also contains parafollicular cells (C-cells). They are located on the outer surface of the follicles, are neuroendocrine cells, do not absorb iodine and belong to the APUD system.
The thyroid gland secretes two iodine-containing hormones, thyroxine (T4) and triiodothyronine (T3), and one peptide hormone, calcitonin.
Thyroxine and triiodothyronine are synthesized in the apical part of the thyroid epithelium and partly in the intrafollicular space, where they accumulate and become part of thyroglobulin. Calcitonin (thyreocalcitonin) is produced by C-cells of the thyroid gland, as well as by the parathyroid glands and the thymus gland.
Follicular cells of the thyroid gland have a unique ability to capture iodine from the bloodstream, which, with the participation of the peroxidase farmer, binds to colloid thyroglobulin. Thyroglobulin plays the role of an intrafollicular reserve of thyroid hormones. If necessary, by pinocytosis, a certain amount of it enters the follicular cell, where, as a result of proteolysis, T3 and T4 are released from thyroglobulin and separated from other hormonally inactive iodinated peptides.
free hormones enter the blood, and iodine proteins undergo deiodization; The released iodine is used for the synthesis of new thyroid hormones. The rate of thyroglobulin breakdown, synthesis of thyroid hormones depends both on the central regulation and on the level of iodine and blood and the presence in it of substances that affect iodine metabolism (immunostimulating globulins, thiocyanates, bromides, etc.). Thus, their synthesis and secretion are carried out at such a rate and in such quantity that the body needs to maintain the concentration of hormones in the tissues that provide homeostasis. The latter is achieved by a complex system of central and peripheral regulation.
Central regulation is carried out by the production of thyroliberin (a releasing factor of thyroid-stimulating hormone) and, possibly, thyreostatin (a factor that inhibits the synthesis of thyroid-stimulating hormone). Thyroid stimulating hormone (TSH) is synthesized by thyrotrophs of the anterior pituitary gland, it stimulates growth and functional activity thyroid epithelium.
The entry of TSH into the blood is regulated by the level of concentration of thyroid hormones in the blood and thyreoliberin, however, the main regulatory factor is the concentration of thyroid hormones in the blood; extremely high level the latter makes thyreotrophs resistant to thyreoliberin.
Peripheral regulation of thyroid metabolism depends on the number of specific receptors for thyroid hormones in the cell; under conditions of a high content of thyroid hormones, their number is reduced, with a low content - increases. Besides, most of thyroxine can be metabolized into an inactive form and thus carry out one of the types of peripheral regulation of the functional state of the body.
The physiological content of thyroid hormones is necessary for the normal synthesis of proteins in various organs and tissues (from the central nervous system to bone tissue); their excess leads to uncoupling of tissue respiration and oxidative phosphorylation in cell mitochondria, followed by a sharp decrease in energy reserve organism.
In addition, by increasing the sensitivity of receptors to catecholamines, thyroid hormones cause an increase in the excitability of the autonomic nervous system, manifested by tachycardia, arrhythmia, increased systolic blood pressure, and increased motility. gastrointestinal tract and secretion of digestive juices: they also increase the breakdown of glycogen, inhibit its synthesis in the liver, affect lipid metabolism. Deficiency of thyroid hormones causes a sharp decline the speed of all oxidative processes in the body and the accumulation of glycosaminoglycans. The cells of the c.n.s. are most sensitive to these changes. myocardium, endocrine glands.
RESEARCH METHODS
Examination of patients with pathology of the thyroid gland includes clinical, laboratory methods for assessing its functional activity, as well as methods for intravital (preoperative) study of the structure of the gland. Palpation of the thyroid gland determines its size, consistency and the presence or absence of nodular formations. Most informative laboratory methods determination of thyroid hormones in the blood are radioimmune methods carried out using standard test kits.
The functional state of the thyroid gland is determined by the absorption of 131I or 99mTc pertechnetate. Methods for in vivo assessment of the structure of the thyroid gland include computed tomography, ultrasound diagnostics, radionuclide scanning and scintigraphy, which provide information on the topography, size and nature of the accumulation of the radiopharmaceutical in various parts of the gland, as well as puncture (aspiration) biopsy followed by microscopy of the punctate.
PATHOLOGY
Clinical manifestations of thyroid diseases are due either to excessive or insufficient production of thyroid hormones, or excessive production of calcitonin and prostaglandins (for example, in medullary carcinoma - a calcitonin-producing tumor), as well as symptoms of compression of the tissues and organs of the neck of an enlarged thyroid gland without impaired hormone production (euthyroidism).
There are five degrees of enlargement of the thyroid gland: O degree - the gland is not visible during examination and is not determined by palpation; I degree - when swallowing, the isthmus is visible, which is determined by palpation, or one of the lobes of the thyroid gland and the isthmus are palpated; II degree - both lobes are palpated, but during examination, the contours of the neck are not changed; III degree- the thyroid gland is enlarged due to both lobes and the isthmus, visible when viewed as a thickening on the anterior surface of the neck (thick neck); Grade IV - large goiter, not sharply asymmetric, with signs of compression of nearby tissues and organs of the neck; V degree - a goiter of extremely large sizes.
Developmental defects. Aplasia (absence) of the thyroid gland is rare, due to a violation of the differentiation of the embryonic rudiment of the thyroid tissue: it is detected in early childhood on the basis of the clinical picture of severe congenital hypothyroidism.
Congenital hypoplasia of the thyroid gland develops due to a lack of iodine in the mother's body, clinically manifested by cretinism and a delay in the physical development of the child. The main type of treatment for both pathological conditions is lifelong hormone replacement therapy.
With preservation of the thyroid duct, often formed median cysts and fistulas of the neck, as well as goiter of the root of the tongue, to be removed. The displacement of the rudiment of the thyroid gland into the mediastinum leads to the development of a retrosternal goiter or tumor. The source of their formation can also be foci of thyroid tissue dystopian in the wall of the trachea, pharynx, myocardium, pericardium.
Injuries to the thyroid gland are extremely rare, they are usually combined with injuries to other organs of the neck. As a rule, injuries are open, accompanied by profuse bleeding, require urgent surgical care. Closed damage observed with compression of the neck (for example, a loop during a suicide attempt), are manifested by the formation of a hematoma.
DISEASES
Among the diseases of the thyroid gland, the most common goiter is diffuse toxic and autoimmune thyroiditis, which are considered as typical. autoimmune diseases with a similar pathogenesis, but a different clinical picture, are often found in blood relatives. The group of infectious inflammatory diseases of the thyroid gland combines different clinical manifestations pathological conditions characterized common symptoms associated with compression of the tissues and organs surrounding the thyroid gland.
Tumors. characteristic benign epithelial tumors thyroid gland, are adenomas of various histological structure. Clinical detection adenomas are based on palpation of the tumor in the thyroid gland with clear contours and a smooth surface that slowly increases in size over time.
The cervical lymph nodes are intact, the function of the gland is most often not changed. In an outpatient setting in the recognition benign tumors in addition to palpation, an important role is played by scanning of the thyroid gland, ultrasound examination, followed by a cytological examination of the punctate. The basic principle of liver surgery is to remove the lobe of the gland in which the tumor is located (hemithyroidectomy). The prognosis after surgical treatment of adenomas is favorable.
Malignant tumors of the thyroid gland are the most common various forms cancer and make up 0.5-2.2% of all malignant neoplasms. Other types of thyroid cancer are less common. Precancerous diseases include nodular and mixed goiter, as well as thyroid adenomas.
The development of thyroid cancer is facilitated by a high level of secretion of thyroid-stimulating hormone from the pituitary gland (observed more often in people living in endemic goiter zones) and X-ray or other irradiation of the head and neck, upper mediastinum, carried out for diagnostic and (or) therapeutic purposes in children and adolescents. age. Of particular importance in the development of thyroid cancer is the combination of external irradiation of these areas with internal irradiation with incorporated radionuclides of iodine when contaminated. environment radioactive substances.
Clinically, thyroid cancer usually manifests itself in two ways. More often, a tumor in the thyroid gland and the presence (or absence) of regional (lymph nodes of the anterolateral neck, supraclavicular and subclavian regions, as well as the anterior superior mediastinum) and distant (lungs, bones, etc.) metastases are determined. On palpation in the gland, a dense, bumpy, often poorly displaced tumor is noted, which over time leads to a change in voice, impaired breathing or swallowing.
In the second clinical variant, the tumor, due to its small size, is not detected by palpation, as well as by radionuclide and ultrasound methods (“hidden cancer” of the thyroid gland); metastases in regional lymph nodes and (or) in distant organs come to the fore. The so-called highly differentiated follicular cancer(malignant adenoma, Langhans metastasizing struma, angioinvasive adenoma), which, with a relatively mature structure, has invasive growth and the ability to metastasize.
Diagnosis of thyroid cancer is very difficult in the presence of long-term existing goiter or adenomas, the leading signs of malignancy of which are their rapid increase, thickening, the appearance of tuberosity, and then limiting the displacement of the gland. The final diagnosis is established only by cytological or histological examination.
At " hidden cancer» along with the determination of the level of calcitonin (medullary cancer), the final stage of diagnosis is often a wide exposure and revision of the thyroid gland. The differential diagnosis of thyroid tumors is based on clinical and radiological findings, the results of a thyroid scan, ultrasound, and computed tomography, targeted puncture of the tumor and subsequent cytological examination punctate.
Surgical treatment includes hemithyroidectomy, subtotal resection of the thyroid gland and thyroidectomy. In the presence of regional metastases on the neck, a fascial-sheath excision of the tissue of the neck is performed. In the presence of distant metastases locally operable cancer, thyroidectomy followed by radioactive iodine treatment is indicated.
The prognosis is favorable for differentiated forms of cancer (follicular and papillary) and unfavorable for other forms. Prevention of thyroid cancer is aimed primarily at the treatment of goiter and benign tumors, with the exception of x-ray exposure and radiotherapy area of the thyroid gland in children and adolescents, preventing the ingress of iodine radionuclides into the body with food and water.
AT early detection thyroid cancer, a large role is given to the clinical examination of patients with various forms of goiter and their surgical treatment, as well as examination of blood relatives of patients suffering from medullary cancer thyroid gland, especially in cases of Sipple's syndrome and mucosal neurinoma syndrome in combination with adenomatosis of the endocrine glands.
Operations on the thyroid gland are performed as under local anesthesia and under intubation anesthesia. Patients with thyrotoxicosis before surgery require special preoperative preparation. The most convenient access to the thyroid gland is a transverse arcuate incision along the anterior surface of the neck 1-1.5 cm above the jugular notch. Retrosternal forms of goiter in most cases can also be removed through this access, although sometimes it is necessary to resort, as in patients with intrathoracic goiter, to thoracotomy.
The main characteristics of each operation on the thyroid gland are the scope of intervention and the method (method) of removal of thyroid tissue. There are intracapsular, intrafascial and extrafascial methods. The intracapsular method is usually used for enucleation of thyroid nodules in order to maximize the preservation of unchanged gland tissue.
Intrafascial secretion of the thyroid gland is used in all forms of goiter, while there is no possible traumatization of the branches of the recurrent laryngeal nerves and the parathyroid glands located outside (rarely inside) the visceral sheet of the 4th fascia of the neck, within which the operation is performed. Sometimes this method is supplemented with ligation of the arteries throughout. The extrafascial method is carried out exclusively in oncological practice and, as a rule, involves ligation of the main arteries of the thyroid gland.
Volume surgical intervention depends on the nature and localization of the pathological process, the size of the pathological focus and the amount of tissue left. The most commonly used partial, subtotal resection and extirpation ( complete removal) of one or both lobes of the thyroid gland. Partial resection is used for small nodular benign goiters, while approximately half of the resected lobe(s) is preserved.
Subtotal resection involves leaving 4 to 8 g of gland tissue in each lobe (usually on the lateral surface of the trachea in the region of the recurrent laryngeal nerves and parathyroid glands). Such interference is performed for all forms of goiter in patients with thyrotoxicosis, as well as for nodular and multinodular euthyroid goiters, which occupy almost the entire lobe (lobes) of the thyroid gland.
Extirpation is used, as a rule, for malignant neoplasms of the thyroid gland, this operation can be supplemented, depending on the stage and localization of the process, by removing the muscles adjacent to the gland, the external and internal jugular veins with tissue containing lymph nodes.
Among possible complications developing after operations on the thyroid gland, paresis of the recurrent laryngeal nerves and hypoparathyroidism, as well as secondary bleeding in the early postoperative period, should be noted.
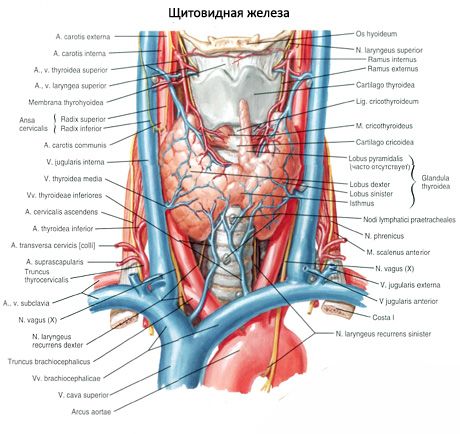
Thyroid (glandula thyroidea) is an unpaired organ located in the anterior region of the neck at the level of the larynx and upper trachea. The gland consists of two lobes - the right (lobus dexter) and the left (lobus sinister), connected by a narrow isthmus. The thyroid gland lies rather superficially. In front of the gland, below the hyoid bone, there are paired muscles: sternothyroid, sternohyoid, scapular-hyoid, and only partly sternocleidomastoid, as well as superficial and pretracheal plates of the cervical fascia.

The posterior concave surface of the gland covers the front and sides of the lower sections of the larynx and upper part trachea. The isthmus of the thyroid gland (isthmus glandulae thyroidei), connecting the right and left lobes, is usually located at level II or III of the tracheal cartilage. AT rare cases the isthmus of the gland lies at the level of the I cartilage of the trachea or even the cricoid arch. Sometimes the isthmus may be absent, and then the lobes of the gland are not connected to each other at all.
The upper poles of the right and left lobes of the thyroid gland are located slightly below the upper edge of the corresponding plate of the thyroid cartilage of the larynx. The lower pole of the lobe reaches the level of the V-VI cartilage of the trachea. The posterolateral surface of each lobe of the thyroid gland is in contact with the laryngeal part of the pharynx, the beginning of the esophagus and the anterior semicircle of the common carotid artery. The parathyroid glands are adjacent to the posterior surface of the right and left lobes of the thyroid gland.
From the isthmus or from one of the lobes, the pyramidal lobe (lobus pyramidalis) extends upward and is located in front of the thyroid cartilage, which occurs in about 30% of cases. This lobe with its apex sometimes reaches the body of the hyoid bone.
The transverse size of the thyroid gland in an adult reaches 50-60 mm. The longitudinal size of each share is 50-80 mm. The vertical size of the isthmus ranges from 5 to 2.5 mm, and its thickness is 2-6 mm. The mass of the thyroid gland in adults from 20 to 60 years is on average 16.3-18.5 g. After 50-55 years, there is a slight decrease in the volume and mass of the gland. The mass and volume of the thyroid gland in women is greater than in men.
Outside, the thyroid gland is covered with a connective tissue sheath - fibrous capsule(capsula fibrosa), which is fused with the larynx and trachea. In this regard, when the larynx moves, the thyroid gland also moves. Inside the gland, connective tissue septa extend from the capsule - trabeculae, dividing the tissue of the gland into lobules, which consist of follicles. The walls of the follicles are lined from the inside with cubic-shaped epithelial follicular cells (thyrocytes), and inside the follicles there is a thick substance - a colloid. The colloid contains thyroid hormones, which consist mainly of proteins and iodine-containing amino acids.
The walls of each follicle (there are about 30 million of them) are formed by a single layer of thyrocytes located on the basement membrane. The size of the follicles is 50-500 microns. The shape of thyrocytes depends on the activity of synthetic processes in them. The more active the functional state of the thyrocyte, the higher the cell. Thyrocytes have a large nucleus in the center, a significant number of ribosomes, a well-developed Golgi complex, lysosomes, mitochondria, and secretion granules in the apical part. The apical surface of thyrocytes contains microvilli immersed in a colloid located in the cavity of the follicle.
The glandular follicular epithelium of the thyroid gland, more than other tissues, has a selective ability to accumulate iodine. In the tissues of the thyroid gland, the concentration of iodine is 300 times higher than its content in the blood plasma. Thyroid hormones (thyroxine, triiodothyronine), which are complex compounds of iodinated amino acids with protein, can accumulate in the colloid of follicles and, as necessary, be released into the bloodstream and delivered to organs and tissues.
Thyroid hormones
Thyroid hormones regulate metabolism, increase heat transfer, enhance oxidative processes and the consumption of proteins, fats and carbohydrates, promote the release of water and potassium from the body, regulate growth and development processes, activate the activity of the adrenal glands, sex and mammary glands, have a stimulating effect on the activity of the central nervous system.
Between the thyrocytes on the basement membrane, as well as between the follicles, there are parafollicular cells, the tops of which reach the lumen of the follicle. Parafollicular cells have a large rounded nucleus, big number myofilaments in the cytoplasm, mitochondria, Golgi complex, granular endoplasmic reticulum. These cells contain many granules of high electron density with a diameter of about 0.15 µm. Parafollicular cells synthesize thyrocalcitonin, which is an antagonist of parathyroid hormone - the hormone of the parathyroid glands. Thyrocalcitonin is involved in the exchange of calcium and phosphorus, reduces the calcium content in the blood and delays the release of calcium from the bones.
The regulation of thyroid function is provided by the nervous system and thyrotropic hormone of the anterior pituitary gland.
Thyroid embryogenesis
The thyroid gland develops from the epithelium of the foregut in the form of an unpaired median outgrowth at a level between I and II visceral arches. Until the 4th week of embryonic development, this outgrowth has a cavity, in connection with which it was called the thyroid duct (ductus thyroglossalis). By the end of the 4th week, this duct atrophies, and its beginning remains only in the form of a more or less deep blind hole at the border of the root and body of the tongue. The distal duct is divided into two rudiments of the future lobes of the gland. The emerging lobes of the thyroid gland are displaced caudally and take their usual position. The preserved distal part of the thyroid-lingual duct turns into a pyramidal lobe of the organ. Reducing sections of the duct can serve as the beginnings for the formation of additional thyroid glands.

Vessels and nerves of the thyroid gland
To the upper poles of the right and left lobes of the thyroid gland, the right and left upper thyroid arteries (branches of the external carotid arteries), and to the lower poles of these lobes - the right and left lower thyroid arteries (from the thyroid trunks of the subclavian arteries). The branches of the thyroid arteries form numerous anastomoses in the capsule of the gland and inside the organ. Sometimes the so-called inferior thyroid artery, which departs from the brachiocephalic trunk, approaches the lower pole of the thyroid gland. Deoxygenated blood from the thyroid gland flows through the superior and middle thyroid veins into the internal jugular vein, along the inferior thyroid vein - into the brachiocephalic vein (or into the lower section of the internal jugular vein).
Lymphatic vessels of the thyroid gland flow into the thyroid, pre-laryngeal, pre- and paratracheal lymph nodes. The nerves of the thyroid gland depart from the cervical nodes of the right and left sympathetic trunks (mainly from the middle cervical node, go along the vessels), as well as from the vagus nerves.



