Sagging heart valve. Various heart diseases that disrupt the normal structure of the valves. Why does pathology develop
During preventive examinations, ultrasound examination of the heart for various reasons, doctors often make a verdict about the presence of MVP. Therefore, many people begin to worry about the question: mitral valve prolapse - what is it, what is dangerous, is it possible to cure it and how. Let's try to figure it out.
Mitral valve prolapse: what is it, what is dangerous
Sagging, bulging of two or one leaflet of the mitral valve into the left atrium during the expulsion of blood into the aorta from the left ventricle. This is the essence of the pathology - mitral valve prolapse. Doctors do not define such a condition as heart disease and call it a developmental feature. As a rule, it is genetically determined and associated with dysplasia. connective tissue.
The danger of prolapse is determined
- functional disorders. Normally, during contraction (systole) of the left ventricle, the valve leaflets between it and the atrium should be tightly closed. In the case of prolapse at this moment, a reverse flow (regurgitation) of blood into the left atrium is possible. This adds extra volume, and the left sections of the heart begin to suffer from overload, their hypertrophy develops. This subsequently leads to pulmonary hypertension, overload of the right heart, to heart failure.
- Violation of the heart rhythm. Patients note periods of palpitations, discomfort and pain in the chest.
- The possibility of the settlement of infectious agents on the altered valve - the development of infective endocarditis with vegetations on the cusps.
Types of pathology
Classify the types of PMC depending on various factors.
Origin:
- due to congenital and genetic features of the development of connective tissue - primary;
- caused by systemic diseases affecting the connective tissue, neuroendocrine, violating the autonomic regulation of the valves, cardiac, affecting the functions of the myocardium and endocardium - secondary.
Manifestations:
- auscultatory - when listening are determined systolic murmur and clicks;
- mute - no pathology is detected on auscultation.
Degrees of sagging of the leaves in mm:
- the first - 3-6;
- the second - 6-9;
- the third is more than 9.
Depths of back flow of blood into the atrium:
- in the area of the valve;
- 1/3 atrium;
- ½ atrium;
- more than half of the cavity.
Expression of manifestations:
- asymptomatic;
- oligosymptomatic - when observation is necessary;
- clinically significant - subject to treatment.
Mitral valve prolapse symptoms
Most cases of primary prolapse go unnoticed, and sagging valve leaflets are detected during examinations for other diseases. But the retrograde analysis of complaints of patients nevertheless reveals characteristic symptoms.
In the absence of leakage or regurgitation of 1-2 degrees, the presence of pathology may be indicated by various minor ailments, which are usually attributed to violations of the autonomic regulation of tone vascular system:
- discomfort, pain in the chest, in the region of the heart, not related to physical activity;
- occasional shortness of breath or feeling short of breath;
- irregular rhythm, "fading" of the heart, palpitations;
- fast onset feeling of fatigue;
- unstable mood;
- night and morning headache
- fainting.
Mitral regurgitation of 3-4 degrees leads to significant violations of cardiac hemodynamics. In the absence of correction, symptoms of heart failure gradually increase.
PMK diagnostics
Accurate diagnosis of prolapse allows the doctor to determine the most appropriate tactics for managing the patient: observation or active therapeutic measures.
During examination and questioning:
- The nature of the patient's complaints may lead the doctor to think about the presence of MVP.
- The general appearance of such patients often indicates congenital pathology connective tissue. Usually these are asthenics with long, thin limbs, pathological joint mobility, often with poor eyesight and strabismus.
- On auscultation of the heart, clicks and a systolic murmur are heard as blood flows into the left atrium through open cusps.
With Echo-KG:
- the deflection of the valve, changes in the cusps and chordal apparatus, the degree of prolapse and the depth of the flow of regurgitation into the left atrium are reliably visualized;
- signs of pulmonary hypertension can be seen and myocardial thickness can be measured.
- Rhythm disturbances are recorded, while monitoring the ECG during the day, episodes of accelerated heartbeat can be detected.
Is treatment required for MVP?
MVP, accompanied by only slight regurgitation at the valve level - up to 1 degree and not manifesting clinical symptoms usually does not require treatment. Perhaps the doctor will recommend periodic monitoring by a cardiologist, conducting control Echo-CG. Patients are asked to eliminate or reduce
- heavy physical activity;
- smoking;
- alcohol abuse;
- passion for strong coffee and tea.
It is necessary to establish a regime of work and rest, engage in physiotherapy exercises, take health walks and get enough sleep.
The vegetative symptoms that disturb patients, of course, require adequate correction. Use of drug therapy
- antiarrhythmics;
- antihypertensive drugs;
- drugs that improve the metabolic processes of the myocardium;
- neuroleptics, sedatives, tranquilizers.
Also, during any operations (tooth extraction, palatine tonsils, etc.), patients with mitral valve prolapse are recommended to prescribe antibiotics a wide range to prevent the development of infective endocarditis.
With severe mitral regurgitation therapy to correct the condition
- cardiac glycosides;
- diuretics;
- ACE inhibitors.
A significant violation of the function of the valve requires surgical intervention - mitral valve plasty is performed. Often operations are performed using enovascular or endoscopic techniques, conducting
- suturing folds;
- shortening of valve chords;
- ablation of myocardial areas in areas that trigger pathological impulses - arrhythmia.
Open valve replacement surgery is performed in severe concomitant pathology.
Forecast
With MVP, not accompanied by significant regurgitation, the prognosis is favorable, especially if you follow the doctor's recommendations and slightly change your lifestyle towards a healthy one. With such a prolapse, you can engage in some sports, unprofessional swimming.
To a question that is relevant for young people - if a conscript has mitral valve prolapse of the 1st degree, is he taken into the army - the answer is yes, they do. Medical disqualification requires a diagnosis of MVP with significant valve dysfunction or complications. As a rule, these are PMK 2 and 3 degrees.
Mitral valve prolapse with regurgitation up to half or the entire length of the atrium requires treatment and sometimes surgical correction. In this case, the prognosis depends on the joint work of doctors and the patient. With a successful tandem, the prognosis is also favorable. Absence adequate treatment threatens to worsen general health and irreversible consequences.
Pregnant women should deal with the prevention of MVP as a congenital pathology - avoid colds, poor environmental conditions, correct violations metabolic processes manifestations of toxicosis.
You can avoid the progression of an existing pathology if you follow the measures recommended by the doctor and regularly monitor the condition.
Mitral valve prolapse (MVP) - such a diagnosis can often be seen in the results of an ultrasound of the heart. However, do not immediately worry: this species valvular disease is often diagnosed in quite healthy people and requires only periodic monitoring by a cardiologist.
Therapeutic tactics directly depends not only on the severity of prolapse (flexion) of the valve, but also on the degree of regurgitation (volume of reverse blood flow).
Mitral valve prolapse - what is it?
The mitral (bicuspid) valve separates the chambers of the left side of the heart: the atrium and the ventricle. Mitral valve prolapse is the deflection of the valve leaflets at the time of contraction (systole) of the left ventricle.
Pathology is caused by a violation of the structure of the valve (its fibrous layer, less often tendon chords) due to connective tissue dysplasia. In this case, the valve flaps not only bend, but may also not close tightly.
With the contraction of the left ventricle through the remaining lumen of the valve, the blood rushes back into the atrium. This process is called regurgitation.
PMK is most often diagnosed in young people 20-35 years old. It is extremely rare that a deviation in the structure and operation of the mitral valve is found in young children. Among adults, the incidence of pathology ranges from 10-25%, and in the elderly - 50%.
Main reasons valvular defect formation:
- Hereditarily caused connective tissue dysplasia (Marfan and Ehlers-Danlo syndromes) - primary valvular prolapse develops;
- Misaligned osteogenesis leading to deformity chest;
- Rheumatic damage to the heart, inflammatory processes in its membranes, heart attack, chronic heart ischemia, atherosclerosis / valvular ring calcification - secondary prolapse is formed.
According to the severity of the deflection distinguish mitral prolapse:
- 1 degree - the height of the dome-shaped deflection of the valves does not exceed 0.6 cm (the norm is 1-2 mm);
- 2 degrees - bulging up to 0.9 cm;
- 3 degrees - the dome of the sash is more than 0.9 cm high.
prolapse symptoms by degree of regurgitation
The classification of MVP according to the severity of the deflection of the valve leaflets is rather arbitrary. The most important factor influencing the general condition of a person and medical tactics, is the degree of regurgitation (1 - 3 degree), which causes a symptomatic picture of mitral insufficiency.
Mitral valve prolapse grade 0

Even with a rather pronounced deflection, the leaflets close tightly, and the volume of blood from the left ventricle enters the aorta in full (there is no reverse flow into the left atrium).
At the same time, regurgitation of 0 degree does not give any painful symptoms: a person feels completely healthy and does not complain about the work of the heart.

pain on exertion
Mitral valve prolapse and 1 degree regurgitation is diagnosed with minimum volume blood returned to the atrium. The patient does not present any complaints indicating circulatory disorders.
Some patients note the occurrence of pain in the right hypochondrium while running. This is due to insufficient right ventricular functionality to increase the volume of blood flow in the heart. The deviation is fixed during the examination:
- Auscultation - listening to the noise at the apex of the heart and a specific click due to the sharp tension of the relaxed chords during ventricular systole. Clicks are more audible in an upright position, may disappear completely when lying down. Sometimes (not necessarily!) “meow” (squeaks) are heard, which occur when the chords or the valve leaf itself vibrate.
- Echocardiography (ultrasound of the heart) - a small gap between the closed valve leaflets and a fixed volume of blood returning to the atrium.
Mitral valve prolapse grade 2 - mitral insufficiency
With prolapse of the bicuspid valve and 2 degrees of regurgitation on ultrasound (Doppler of the heart), more pronounced signs of mitral insufficiency are recorded. The blood stream, returning through the incompletely closed valve, reaches the middle of the atrial chamber.
More than 25% of the blood returns to the atrium from the ventricle. In this case, symptoms characteristic of stagnation in the pulmonary circulation are observed:
- Cardiac pain - mild to moderate, not closely related to physical exertion or emotional response to stress (may occur spontaneously). Taking Nitroglycerin does not have a special effect in eliminating such pain.
- Headache - intense, often bilateral (only sometimes mimics a migraine). Headache often occurs against the background of a sharp change in the weather, after an emotional overstrain.
- Shortness of breath - often provoked by hyperventilation syndrome (deep or frequent breaths provoked by a feeling of lack of air). Shortness of breath can occur even after minimal physical exertion.
- Autonomic dysfunction - manifested by a lump in the throat, excessive sweating, fatigue and morning weakness, an unreasonable rise in temperature to 37.0-37.5ºС, nausea and dizziness. Wherein vegetative crises are repeated at least once a week, are not associated with situations that threaten the patient, and the emotional side of this state is somewhat muffled. It is also extremely rare for fainting to occur. Vegetative disorders provoke the development of depressive states and emotional instability (sadness and gloom in the morning, anxiety and irritability in the evening). Often, patients complain of specific bodily sensations, which are sometimes perceived as a symptom of another somatic disease.
- Interruptions in the work of the heart - periodically the patient notes tremors or fading of the heart. At the same time, extrasystoles (extraordinary heartbeats) and tachycardia (increased heart rate) are not constantly recorded, but occur during emotional experience, physical exertion, or even after drinking coffee.
Mitral valve prolapse grade 3
Insufficiency in the pulmonary circulation leads to an increase in the load on the right half of the heart. Already existing symptoms are gradually aggravated and severe signs of insufficiency of a large circle appear: edema, increased pressure, cyanosis of the skin, irresistible weakness, atrial fibrillation and liver enlargement. Such patients usually receive 1 disability group.
Mitral valve prolapse is life-threatening precisely with 3 degrees of regurgitation: it is possible to develop paroxysmal tachycardia, pulmonary edema, endocarditis and other serious complications, up to sudden death.
Patients with bicuspid valve prolapse are more likely to suffer from colds, often they are diagnosed with chronic tonsillitis.
- Congenital dysplastic connective tissue pathology in childhood is indicated by dysplastic changes in the hip joints, flat feet, and abdominal hernias.
mitral valve prolapse during pregnancy
A slight prolapse of the bicuspid valve and a slight mitral insufficiency is not a contraindication to pregnancy, the bearing of the child in this case is normal.
In this case, there may even be a temporary decrease in the deflection of the valve leaflets due to a physiological increase in the size of the left ventricle. However, systolic murmur and clicks return 1 month after delivery.
More dangerous is a severe degree of regurgitation and mitral valve prolapse during pregnancy: the risk of developing attacks of paroxysmal tachycardia is significantly increased. During childbirth, a rupture of the valve chords is not excluded.
In women with MVP, premature discharge of amniotic fluid and weakness of labor pains are often recorded. The baby is prone to intrauterine asphyxia and is often born with low weight (hypotrophy).
 Therapeutic tactics is chosen in strict accordance with the degree of bicuspid valve prolapse, the presence / absence of signs of mitral insufficiency and the complications that have arisen.
Therapeutic tactics is chosen in strict accordance with the degree of bicuspid valve prolapse, the presence / absence of signs of mitral insufficiency and the complications that have arisen.
1 degree of mitral valve prolapse: healing measures
With a slight change in the structure of the valves (mitral valve prolapse with regurgitation of the 1st degree), the absence of persistent arrhythmia and other painful symptoms, treatment is not required. A person is recommended to be monitored by a cardiologist once a year and correct the basics of life:
- Quit smoking, alcohol, coffee and strong tea;
- Balanced diet;
- Physical activity, commensurate with the capabilities of the body;
- Education of stress resistance;
- Rational schedule of work - rest.
Treatment of MVP and 2 degrees of regurgitation
The appearance of painful symptoms of mitral valve prolapse indicates the need for drug therapy. The treatment regimen includes:
- Elimination of heart pain - it is advisable to use sedatives (valerian, sage, hawthorn, St. John's wort, motherwort);
- Vegeto therapy vascular dystonia- andidepressants (Amitriptyline, Azafen), neuroleptics (Sonopax, Triftazin), tranquilizers (Elenium, Seduxen, Grandaxin);
- Improvement of metabolism in the myocardium - Riboxin, Kartinin, coenzyme Q-10, Panangin, vitamins and magnesium preparations (especially effective for mitral prolapse!);
- Restoration of the heart rhythm - Obzidan and other adrenergic blockers;
- Prevention of infective endocarditis - broad-spectrum antibiotics for each surgical intervention (tooth extraction, tonsillectomy).
Management of severe regurgitation in bicuspid valve prolapse
To eliminate the progression of the disease and prevent severe consequences mitral insufficiency, cardiac glycosides, diuretics, ACE inhibitors(non-hypotensive dosage of Captopril - about 0.5 mg / kg of body weight per day - has a cardioprotective effect). Simultaneously with drug therapy, surgical plastic surgery of the bicuspid valve is performed.
Depending on the structural changes, cardiac surgeons shorten the valvular chords, suture the leaflets and ablate the foci of pathological impulses (elimination of arrhythmia). In severe cases, it is complete replacement valve.
The possibilities of modern medicine allow many heart surgeries to be performed using endovascular (transcatheter) or endoscopic access. To open operation cardiac surgeons resort only to extreme cases, for example, with combined defects.
Forecast
In the absence of mitral insufficiency, the outcome of the disease is usually favorable. It is worth noting that a slight deflection of the valve leaflets in lean people and adolescent children may disappear on their own if the rest regimen is observed, appropriate physical activity and complete nutrition.
The health of a patient with a severe degree of mitral prolapse and the rapid progression of the disease directly depends on the timeliness and adequacy of medical care.
Heart defects- These are changes in the structure of the heart that cause disturbances in its work. These include defects in the wall of the heart, ventricles and atria, valves, or outgoing vessels. Heart defects are dangerous because they can lead to impaired circulation in the heart muscle itself, as well as in the lungs and other organs, and cause life-threatening complications.
Heart defects are divided into 2 large groups.
- congenital heart defects
- Acquired heart defects
It is believed that 1% of children are born with a defect. In Russia, this amounts to 20,000 people annually. But to these statistics it is necessary to add those cases when congenital malformations are detected after many years. The most common problem is a ventricular septal defect, accounting for 14% of all cases. It happens that at the same time in the heart of a newborn several defects are detected at once, which usually occur together. For example, tetralogy of Fallot is about 6.5% of all newborns with heart defects.
Acquired vices appear after birth. They can be the result of trauma heavy loads or diseases: rheumatism, myocarditis, atherosclerosis. The most common cause of the development of various acquired defects is rheumatism - 89% of all cases.
Acquired heart defects are a fairly common phenomenon. Do not think that they appear only in old age. A large proportion falls on the age of 10-20 years. But still, the most dangerous period is after 50. In old age, 4-5% of people suffer from this problem.
After the past diseases, violations of the heart valves mainly appear, which ensure the movement of blood in the right direction and prevent it from returning back. Most often, problems arise with the mitral valve, which is located between the left atrium and the left ventricle - 50-75%. In second place in the risk group is the aortic valve, located between the left ventricle and the aorta - 20%. The pulmonary and tricuspid valves account for 5% of cases.
Modern medicine has the ability to correct the situation, but surgery is necessary for a complete cure. Medication may improve well-being, but will not eliminate the cause of the disorder.
Anatomy of the heart
In order to understand what changes cause heart disease, you need to know the structure of the organ and the features of its work.Heart- a tireless pump that pumps blood around our body without stopping. This organ is the size of a fist, has the shape of a cone and weighs about 300 g. The heart is divided lengthwise into two halves, right and left. The upper part of each half is occupied by the atria, and the lower part by the ventricles. Thus, the heart consists of four chambers.
Oxygen-poor blood comes from the organs to the right atrium. It contracts and pumps a portion of blood into the right ventricle. And he sends it to the lungs with a powerful push. This is the beginning pulmonary circulation Key words: right ventricle, lungs, left atrium.
In the alveoli of the lungs, the blood is enriched with oxygen and returns to the left atrium. Through the mitral valve, it enters the left ventricle, and from it goes through the arteries to the organs. This is the beginning systemic circulation: left ventricle, organs, right atrium.
First and main condition proper functioning of the heart: blood without oxygen used by organs and blood enriched with oxygen in the lungs should not mix. For this, the right and left halves are normally tightly separated.
The second prerequisite A: Blood should only move in one direction. This is provided by valves that do not allow blood to take "a single step back."
What is the heart made of
The function of the heart is to contract and expel blood. The special structure of the heart helps it pump 5 liters of blood per minute. This is facilitated by the structure of the body.
The heart has three layers.
- Pericardium - outer two-layer bag of connective tissue. Between outer and inner layer there is a small amount of fluid that helps reduce friction.
- Myocardium - middle muscle layer, which is responsible for the contraction of the heart. It consists of special muscle cells that work around the clock and have time to rest in a split second between beats. In different parts, the thickness of the heart muscle is not the same.
- Endocardium - the inner layer that lines the chambers of the heart and forms the septa. Valves are folds of the endocardium along the edges of the holes. This layer consists of strong and elastic connective tissue.
Valve anatomy
The chambers of the heart are separated from each other and from the arteries by fibrous rings. These are layers of connective tissue. They have holes with valves that let blood flow in the right direction, and then close tightly and prevent it from returning back. Valves can be compared to a door that only opens one way.There are 4 valves in the heart:
- mitral valve between the left atrium and the left ventricle. It consists of two valves, papillary or papillary muscles and tendon filaments - chords that connect the muscles and valves. When blood fills the ventricle, it presses on the valves. The valve closes under blood pressure. Tendon chords do not allow the valves to open towards the atrium.
- tricuspid, or tricuspid valve - between the right atrium and the right ventricle. It consists of three valves, papillary muscles and tendon chords. The principle of its operation is the same.
- aortic valve between the aorta and the left ventricle. It consists of three petals, which have a crescent shape and resemble pockets. When blood is pushed into the aorta, the pockets fill up, close, and prevent it from returning to the ventricle.
- Pulmonary valve between the right ventricle and the pulmonary artery. It has three leaflets and works on the same principle as the aortic valve.
The structure of the aorta
It is the largest and most important artery in the human body. It is very elastic, easily stretched due to the large number of elastic connective tissue fibers. An impressive layer of smooth muscles allows it to narrow and not lose its shape. Outside, the aorta is covered with a thin and loose membrane of connective tissue. It carries oxygen-enriched blood from the left ventricle and divides into many branches, these arteries wash all organs.The aorta looks like a loop. It rises up behind the sternum, spreads through the left bronchus, and then goes down. In connection with this structure, 3 departments are distinguished:
- Ascending aorta. At the beginning of the aorta there is a small extension called the aortic bulb. It is located directly above the aortic valve. Above each of its semilunar petals there is a sinus - a sinus. The right and left aorta originate in this part of the aorta. coronary arteries, which are responsible for the nutrition of the heart.
- Aortic arch. Important arteries emerge from the aortic arch: the brachiocephalic trunk, the left common carotid and the left subclavian artery.
- Descending aorta. It is divided into 2 departments: thoracic aorta and abdominal aorta. Numerous arteries depart from them.
While the fetus develops inside the uterus, it has a duct between the aorta and the pulmonary trunk - a vessel that connects them. As long as the child's lungs are not working, this window is vital. It protects the right ventricle from overflow.
Normally, after birth, a special substance is released - bradycardin. It causes the muscles of the arterial duct to contract and it gradually turns into a ligament, a strand of connective tissue. This usually happens within the first two months after birth.
If this does not happen, then one of the heart defects develops - an open ductus arteriosus.
oval hole
The foramen ovale is the door between the left and right atrium. It is necessary for the child while he is in the uterus. During this period, the lungs do not work, but they need to be fed with blood. Therefore, the left atrium, through the foramen ovale, transfers part of its blood to the right, so that there is something to fill the pulmonary circulation.
After childbirth, the lungs begin to breathe on their own and are ready to supply oxygen to a small body. The oval hole becomes unnecessary. Usually it is closed with a special valve, like a door, and then completely overgrown. This happens during the first year of life. If this did not happen, then oval window may remain open throughout life.
Interventricular septum
Between the right and left ventricles there is a septum, which consists of muscle tissue and is covered with a thin layer of connective cells. Normally, it is solid and tightly separates the ventricles. This structure ensures the supply of oxygen-rich blood to the organs of our body.
But some people have a hole in this septum. Through it, the blood of the right and left ventricles is mixed. Such a defect is considered a heart defect.
mitral valve
Mitral valve anatomy The mitral valve is located between the left atrium and the left ventricle. It consists of the following elements:
- atrioventricular ring from connective tissue. It is located between the atrium and the ventricle and is a continuation of the connective tissue of the aorta and the basis of the valve. There is a hole in the center of the ring, its circumference is 6-7 cm.
- Valve flaps. The sashes resemble two doors covering a hole in the ring. The front flap deepens more and resembles a tongue, while the back flap is attached around the circumference and is considered the main one. In 35% of people, it splits, and additional valves appear.
- Tendon chords. These are dense connective tissue fibers resembling threads. In total, 30-70 chords 1-2 cm long can be attached to the valve flaps. They are fixed not only to the free edge of the flaps, but also over their entire surface. The other end of the chords is attached to one of the two papillary muscles. The task of these small tendons is to hold the valve during contraction of the ventricle and prevent the leaflet from opening and releasing blood into the atrium.
- Papillary or papillary muscles. It is an extension of the heart muscle. They look like 2 small papilla-shaped outgrowths on the walls of the ventricle. It is to these papillae that the chords are attached. The length of these muscles in adults is 2-3 cm. They contract together with the myocardium and stretch the tendon filaments. And they firmly hold the valve flaps and do not allow it to open.
mitral valve stenosis
 Mitral valve stenosis is a heart disease that is associated with a narrowing of the valve lumen between the left atrium and the left ventricle. In this disease, the valve leaflets thicken and grow together. And if the normal area of the hole is about 6 cm, then with stenosis it becomes less than 2 cm.
Mitral valve stenosis is a heart disease that is associated with a narrowing of the valve lumen between the left atrium and the left ventricle. In this disease, the valve leaflets thicken and grow together. And if the normal area of the hole is about 6 cm, then with stenosis it becomes less than 2 cm. The reasons
Mitral valve stenosis can be caused by congenital anomalies development of the heart and past diseases.
Birth defects:
- fusion of the valve leaflets
- supravalvular membrane
- reduced annulus
infectious diseases:
- sepsis
- brucellosis
- syphilis
- angina
- pneumonia
Rheumatic (autoimmune) diseases cause 80% of mitral valve stenosis

- rheumatism
- scleroderma
- systemic lupus erythematosus
- dermatopolymyositis
Regardless of what caused the narrowing of the mitral valve, the symptoms of the disease will be the same.
Symptoms
When the mitral valve narrows, pressure rises in the left atrium and in the pulmonary arteries. This explains the disruption of the lungs and the deterioration of oxygen supply to all organs.Normally, the area of the opening between the left atrium and the ventricle is 4-5 cm 2 . With small changes in the valve well-being remains normal. But the smaller the gap between the chambers of the heart, the worse the condition of the person.
With a narrowing of the lumen twice to 2 cm 2, the following symptoms appear:
- weakness that gets worse when walking or performing daily activities;
- increased fatigue;
- dyspnea;
- irregular heartbeat - arrhythmia.
- cough and hemoptysis after active loads and at night;
- swelling in the legs;
- pain in the chest and in the region of the heart;
- bronchitis and pneumonia often occur.
Mitral valve stenosis symptoms:
- the skin is pale, but a blush appears on the cheeks;
- bluish areas appear on the tip of the nose, ears and chin (cyanosis);
- attacks of atrial fibrillation, with a strong narrowing of the lumen, arrhythmia can become permanent;
- swelling of the limbs;
- "heart hump" - protrusion of the chest in the region of the heart;
- strong beats of the right ventricle against the chest wall are heard;
- "Cat's purr" occurs after squats, in a position on the left side. The doctor puts his hand on the patient's chest and feels how the blood oscillates through the narrow opening of the valve.
- The most characteristic feature is diastolic murmur. It occurs during the relaxation phase of the ventricles in diastole. This noise appears due to the fact that the blood rushes at high speed through the narrow opening of the valve, turbulence appears - the blood flows with waves and swirls. Moreover, the smaller the diameter of the hole, the louder the noise.
- If in adults, normal heart contraction consists of two tones:
- 1 ventricular contraction sound
- 2 the sound of closing the valves of the aorta and pulmonary artery.
 Electrocardiogram (ECG).
Reveals an increase in the left atrium and right ventricle. It also makes it possible to assess whether there are heart rhythm disturbances - arrhythmia.
Electrocardiogram (ECG).
Reveals an increase in the left atrium and right ventricle. It also makes it possible to assess whether there are heart rhythm disturbances - arrhythmia.
Phonocardiogram (PCG). With mitral valve stenosis, a graphic recording of heart sounds appears:
- characteristic noises that are heard before the contraction of the ventricles. It is created by the sound of blood passing through a narrow opening;
- "click" of the closing mitral valve.
- the jerky "pop" that the ventricle creates when it pushes blood into the aorta.
- enlargement of the left atrium;
- valve seal;
- the valve leaflets close more slowly than in a healthy person.
Diagnostics
The process of establishing a diagnosis begins with a questioning of the patient. The doctor asks about the manifestations of the disease and conducts an examination.The following objective symptoms are considered direct evidence of mitral valve stenosis:
- noise of blood while it fills the ventricles;
- "click" that is heard during the opening of the mitral valve;
- trembling of the chest, which is caused by the passage of blood through the narrow opening of the valve and the vibration of its valves - "cat's purr".
- X-rays show dilated veins, arteries, and a displaced esophagus to the right.
- An electrocardiogram shows left atrial enlargement.
- The phonocardiogram reveals a murmur during diastole (relaxation of the heart muscle) and a click from the closing of the valve.
- The echocardiogram shows a slowdown in the valve and an increase in the heart.
Treatment
By using medicines it is impossible to eliminate heart disease, but it is possible to improve blood circulation and the general condition of a person. For these purposes, various groups of drugs are used.- Cardiac glycosides: Digoxin, Celanide These funds help the heart contract more intensively and slow down the frequency of beats. They are especially necessary for you if the heart cannot cope with the load and starts to hurt. Digoxin is taken 4 times a day, 1 tablet. Celanide - one tablet 1-2 times a day. The course of treatment is 20-40 days.
- Diuretics (diuretics): Furosemide, Veroshpiron They increase the rate of urine production and help remove excess water from the body, reduce pressure in the vessels of the lungs and in the heart. Usually prescribed 1 diuretic tablet in the morning, but the doctor can increase the dose several times if the need arises. The course is 20-30 days, then they take a break. Together with water, useful minerals and vitamins are removed from the body, so it is advisable to take a vitamin-mineral complex, for example, Multi-Tabs.
- Beta-blockers: Atenolol, Propranolol They help to return the rhythm of the heart to normal if there is atrial fibrillation or other rhythm disturbances. They reduce the pressure in the left atrium during exercise. Take 1 tablet before meals without chewing. Minimum exchange rate 15 days, but usually the doctor prescribes long-term treatment. It is necessary to cancel the drug gradually so as not to cause deterioration.
- Anticoagulants: Warfarin, Nadroparin You need them if a heart defect has caused left atrial enlargement, atrial fibrillation, which increases the risk of blood clots forming in the atrium. These drugs thin the blood and prevent the formation of blood clots. Take 1 tablet 1 time per day at the same time. For the first 4-5 days, a double dose of 5 mg is prescribed, and then 2.5 mg. Treatment lasts 6-12 months.
- Anti-inflammatory and antirheumatic drugs: Diclofenac, Ibuprofen
These non-steroidal anti-inflammatory drugs relieve pain, inflammation, swelling, and lower the temperature. They are especially needed for those whose heart disease caused rheumatism. Take 25 mg 2-3 times a day. Course up to 14 days.
Remember that every medicine has its own contraindications and can cause serious side effects. Therefore, do not self-medicate and do not take drugs that have helped your friends. Only an experienced doctor can decide which medicines you need. At the same time, it takes into account whether the drugs you are taking will be combined.
Types of operations for mitral valve stenosis
Surgery in childhood Whether surgery is needed for congenital mitral valve stenosis, the doctor decides depending on the condition of the child. If the cardiologist has determined that it is impossible to do without urgent elimination of the problem, then the baby can be operated on immediately after birth. If there is no danger to life, and there is no developmental delay, then the operation can be performed at the age of up to three years or postponed to a later date. Such treatment will allow the baby to develop normally and in no way lag behind their peers.
Whether surgery is needed for congenital mitral valve stenosis, the doctor decides depending on the condition of the child. If the cardiologist has determined that it is impossible to do without urgent elimination of the problem, then the baby can be operated on immediately after birth. If there is no danger to life, and there is no developmental delay, then the operation can be performed at the age of up to three years or postponed to a later date. Such treatment will allow the baby to develop normally and in no way lag behind their peers.
Mitral valve repair.
If the changes are small, then the surgeon will cut the fused sections of the valves and expand the lumen of the valve.
Mitral valve replacement. If the valve is severely damaged or there are developmental anomalies, the surgeon will put a silicone prosthesis in its place. But after 6-8 years, the valve will need to be replaced.
Indications for surgery for congenital mitral valve stenosis in children
- the area of the opening in the mitral valve is less than 1.2 cm 2 ;
- severe developmental delay;
- a strong increase in pressure in the vessels of the lungs (pulmonary circulation);
- deterioration of well-being, despite the constant use of drugs.
- severe heart failure;
- thrombosis of the left atrium (you must first dissolve the blood clots with anticoagulants);
- severe damage to several valves;
- infective endocarditis inflammation of the inner lining of the heart;
- exacerbation of rheumatism.
Balloon valvuloplasty
 This operation is performed through a small incision in the femoral vein or artery. A balloon is inserted through it into the heart. When it is in the mitral valve opening, the doctor inflates it sharply. The operation is carried out under X-ray and ultrasound control.
This operation is performed through a small incision in the femoral vein or artery. A balloon is inserted through it into the heart. When it is in the mitral valve opening, the doctor inflates it sharply. The operation is carried out under X-ray and ultrasound control.
- the area of the mitral valve opening is less than 1.5 cm 2;
- coarse deformation of the valve leaflets;
- sashes retain their mobility;
- there is no significant thickening and calcification of the valves.
- rarely gives complications;
- immediately after the operation, shortness of breath and other phenomena of circulatory failure disappear;
- it is considered a low-traumatic method and makes it easier to recover after surgery;
- recommended for all patients with minor changes in the valve;
- gives nice results even if the valve blades are deformed.
- cannot eliminate serious changes in the valve (calcification, deformation of the valves);
- should not be performed with severe damage to several heart valves and left atrial thrombosis;
- the risk that a second operation will be required reaches 40%.
Transthoracic commissurotomy. This is an operation that allows you to cut the adhesions on the valve leaflets, which narrow the lumen between the left atrium and ventricle. The operation can be performed through the femoral vessels using a special flexible catheter that reaches the valve. Another option is to make a small incision on the chest and to the mitral valve through the interatrial sulcus lead a surgical instrument, which expands the opening of the valve. This operation is performed without a heart-lung machine.
Indications for this type of operation
- the size of the mitral valve duct is less than 1.2 cm 2 ;
- the size of the left atrium reached 4-5 cm;
- increased venous pressure;
- there is stagnation of blood in the vessels of the lungs.
- gives good results;
- does not require artificial circulation, when the blood pumps the device through the body, and the heart is excluded from the circulatory system;
- a small incision on the chest heals quickly;
- well tolerated.
The operation is ineffective if there is a thrombus in the left atrium, mitral valve calcification or lumen narrowed too much. In this case, you will have to make an incision between the ribs, apply artificial blood circulation and carry out open commissurotomy.
Open commissurotomy
Indications for this type of operation
- the diameter of the mitral valve opening is less than 1.2 cm;
- mild to moderate mitral insufficiency;
- calcification and low mobility of the valve.
- gives good results of treatment;
- allows you to reduce pressure in the atrium and pulmonary veins;
- the doctor sees what changes have occurred in the structures of the valve;
- if during the operation it turns out that the valve is badly damaged, then you can immediately put an artificial one;
- can be performed if there is a thrombus in the left atrium or several valves are affected;
- effective when balloon valvuloplasty and transthoracic commissurotomy failed.
- the need for artificial circulation;
- a large incision on the chest heals longer;
- 50% of people have stenosis again within 10 years after surgery.
 Doctors can supply a mechanical mitral valve made from silicone, metal, and graphite. It is durable and does not wear out. But such valves have one drawback - they increase the risk of blood clots in the heart. Therefore, after the operation, you will have to take drugs for life to thin the blood and prevent the formation of clots.
Doctors can supply a mechanical mitral valve made from silicone, metal, and graphite. It is durable and does not wear out. But such valves have one drawback - they increase the risk of blood clots in the heart. Therefore, after the operation, you will have to take drugs for life to thin the blood and prevent the formation of clots.
Biological valve prostheses can be donated or from animal hearts. They do not cause blood clots, but wear out. Over time, the valve may burst or calcium accumulates on its walls. Therefore, young people after 10 years will need a second operation.
- women of childbearing age who plan to have children. Such a valve does not cause spontaneous abortions in pregnant women;
- over the age of 60;
- people who cannot tolerate anticoagulant drugs;
- when there are infectious lesions of the heart;
- repeated heart surgeries are planned;
- blood clots form in the left atrium;
- have bleeding disorders.
- narrowing of the valve (less than 1 cm in diameter) if for some reason it is impossible to cut the adhesions between its petals;
- wrinkling of the valves and tendon threads;
- a thick layer of connective tissue (fibrosis) has formed on the valve flaps and they do not close well;
- there are large deposits of calcium on the valve leaflets.
- the new valve makes it possible to completely solve the problem, even in patients with severe changes in the valve;
- the operation can be performed at a young age and after 60 years;
- re-stenosis does not occur;
- after recovery, the patient will be able to lead a normal life.
- it is necessary to exclude the heart from the circulatory system and immobilize it.
- it takes about 6 months for full recovery.
Mitral valve prolapse
 Mitral valve prolapse(PMC) or Barlow's syndrome is a heart disease in which the leaflets of the mitral valve bend into the left atrium during the contraction of the left ventricle. In this case, a small amount of blood returns to the atrium. She joins a new portion, which comes from two pulmonary veins. This phenomenon is called "regurgitation" or "reverse reflux".
Mitral valve prolapse(PMC) or Barlow's syndrome is a heart disease in which the leaflets of the mitral valve bend into the left atrium during the contraction of the left ventricle. In this case, a small amount of blood returns to the atrium. She joins a new portion, which comes from two pulmonary veins. This phenomenon is called "regurgitation" or "reverse reflux". This disease is present in 2.5-5% of people and most of them do not even know about it. If the changes in the valve are minor, then there are no symptoms of the disease. In this case, doctors consider mitral valve prolapse to be a variant of the norm - a feature of the development of the heart. Most often it is found in young people under 30 years old, and in women several times more often.
It is believed that with age, changes in the valve may disappear on their own. But in any case, if you have mitral valve prolapse, then you need to visit a cardiologist at least once a year and do an ultrasound of the heart. This will help to avoid heart rhythm disturbances and infective endocarditis.
Reasons for the appearance of PMK
Doctors identify congenital and acquired causes of prolapse.Congenital
- disturbed structure of the mitral valve cusps;
- weakness of the connective tissue that makes up the valve;
- too long tendon chords;
- violations of the structure of the papillary muscles, to which the chords are attached, fixing the valve.
infectious diseases
- angina
- scarlet fever
- sepsis
Autoimmune pathologies
- rheumatism
- scleroderma
- red systemic lupus
Other reasons
- strong blows to the chest can cause a rupture of the notochord. In this case, the valve flaps will also not close tightly.
- consequences of myocardial infarction. When the work of the papillary muscles responsible for closing the valves is disrupted.
Symptoms
20-40% of people diagnosed with mitral valve prolapse have no symptoms of the disease. This means that little or no blood seeps into the atrium.
PMK often occurs in tall, slender people, they have long fingers, a depressed chest, and flat feet. Such structural features of the body are often accompanied by prolapse.
In some cases well-being may worsen. This usually happens after strong tea or coffee, stress or activity. In this case, a person may feel:
- pain in the region of the heart;
- strong heartbeat;
- weakness and faintness;
- bouts of dizziness;
- increased fatigue;
- bouts of fear and anxiety;
- heavy sweating;
- shortness of breath and feeling short of breath;
- fever not associated with infectious diseases.
- tachycardia - the heart beats faster than 90 beats per minute;
- arrhythmia - the appearance of extraordinary "unplanned" heart contractions against the background of normal rhythm;
- rapid breathing;
- systolic trembling - trembling of the chest, which the doctor feels at hand during probing. It is created by vibrating valve flaps when a stream of blood breaks through a narrow gap between them under high pressure. This happens at the moment when the ventricles contract and the blood, through small defects in the valves, returns to the atrium;
- tapping (percussion) may reveal that the heart is constricted.
Listening to the heart with a stethoscope gives the doctor the opportunity to identify such violations: - systolic murmur. It is produced by blood leaking through the valve back into the atrium during ventricular contraction;
- instead of two tones during heart contraction (I - the sound from the contraction of the ventricles, II - the sound from the closing of the valves of the aorta and pulmonary arteries), as in people with a healthy heart, you can hear three tones - “quail rhythm”. The third element of the melody is the click of the mitral valve petals at the moment of closing;
Regardless of whether congenital or acquired MVP, it is felt by a person in the same way. Symptoms of the disease depend on the general condition of cardio-vascular system and the amount of blood that leaks back into the atrium.
Instrumental examination data
Electrocardiogram. With MVP, Holter monitoring is often used, when a small sensor constantly records the cardiogram of the heart for several days while you are doing your business as usual. It can detect heart rhythm disturbances (arrhythmia) and untimely contraction of the ventricles (ventricular extrasystoles).Two-dimensional echocardiography or ultrasound of the heart. Reveals that one or both leaflets of the valve bulge, bend towards the left atrium and during contraction they move back. You can also determine how much blood is returning from the ventricle to the atrium (what is the degree of regurgitation) and whether there are changes in the valve leaflets themselves.
Chest x-ray. May show that the heart is normal or reduced in size, sometimes there is an expansion of the initial section of the pulmonary artery.
Diagnostics
In order to correctly diagnose the doctor listens to the heart. Characteristic signs of mitral valve prolapse:
- click of the valve leaflets during the contraction of the heart;
- the sound of blood passing through a narrow gap between the valve leaflets in the direction of the atrium.
- bulging of the mitral valve leaflets, they look like rounded baths;
- flow of blood from the ventricle to the atrium more blood returns, the worse the state of health;
- valve thickening.
There are no drugs that can cure mitral valve prolapse. If the form is not severe, then treatment is not required at all. It is advisable to avoid situations that provoke heart attacks, drink tea, coffee, and alcoholic beverages in moderation.
Drug treatment is prescribed if your health worsens.
- Calming drugs (sedatives) Preparations based on medicinal herbs: tinctures of valerian, hawthorn or peony. They not only calm the nervous system, but also improve the functioning of blood vessels. These drugs help to get rid of the manifestations of vegetative-vascular dystonia, which affects all those who have mitral valve prolapse. Tinctures can be taken for a long time, 25-50 drops 2-3 times a day.
- Tranquilizers: Diazepam Helps relieve anxiety, fear and irritability. It improves sleep and slows down the heart rate. Take half a tablet or a whole 2-4 times a day. The duration of treatment is 10-14 days. The drug can not be combined with other sedatives and alcohol, so as not to overload the nervous system.
- B-blockers: Atenolol Reduces the effect of adrenaline on nerve receptors, thereby reducing the effect of stress on blood vessels and the heart. It balances the effect on the heart of the sympathetic and parasympathetic nervous systems that control the frequency of contractions, while the pressure in the vessels decreases. Relieves arrhythmias, palpitations, dizziness and migraines. Take 1 tablet (25 mg) once a day before meals. If this is not enough, the doctor will increase the dose. The course of treatment is 2 weeks or more.
- Antiarrhythmic drugs: Magnesium orotate Magnesium in its composition improves the production of collagen and thereby strengthens the connective tissue that makes up the valve. It also improves the ratio of potassium, calcium and sodium, and this leads to a normal heart rhythm. Take 1 g daily for a week. Then the dose is halved to 0.5 g and continue to drink for 4-5 weeks. Should not be taken by people with kidney disease and children under 18 years of age.
- Means for lowering pressure: Prestarium, Captopril
Inhibit the action of a specific enzyme, causing an increase pressure. Restore the elasticity of large vessels. Do not allow the atria and ventricles to stretch from increased blood pressure. Improve the condition of the connective tissue of the heart and blood vessels. Prestarium take 1 tablet (4 mg) 1 time per day in the morning. After a month, the dose can be increased to 8 mg and taken with diuretics. Treatment, if necessary, can continue for years.
Combined drugs: Corvalol, Valoserdin will help reduce the frequency of heart contractions and make attacks of the disease more rare. These medicines are drunk daily 2-3 times a day. Usually the course is 2 weeks. After 7 days of rest, the treatment can be repeated. Do not abuse these drugs, addiction and disorders of the nervous system may occur. Therefore, always follow the dose exactly.
Surgery for mitral valve prolapse
Surgery for MVP is extremely rare. Depending on your state of health, age and degree of valve damage, the surgeon will suggest one of the existing techniques.Balloon valvuloplasty
The operation can be performed under local anesthesia. A flexible cable is inserted through a large vessel of the thigh, which, under X-ray control, is advanced to the heart and stopped in the lumen of the mitral valve. The balloon is inflated, thus expanding the valve opening. At the same time, its sashes are aligned.
Indications for this type of operation
- a large volume of blood that returns to the left atrium;
- constant deterioration of well-being;
- drugs do not help relieve the symptoms of the disease;
- increased pressure in the left atrium by more than 40 mm Hg.
- carried out under local anesthesia;
- easier to bear than surgery open heart;
- no need to stop the heart for the period of the operation and connect the heart-lung machine;
- faster and easier recovery period.
- should not be performed if there are problems with other valves or right ventricular failure;
- high risk the fact that within 10 years the disease will return, there will be a relapse.
This operation to replace a damaged heart valve with an artificial one is performed very rarely, because MVP is considered a relatively mild pathology. But in exceptional cases Your doctor will recommend a mitral valve prosthesis. It can be biological (human, pig, horse) or artificial, created from silicone and graphite.
Indications for this type of operation
- a sharp deterioration in the condition;
- heart failure;
- rupture of the chord that holds the valve leaflets.
- eliminates the recurrence of the disease;
- allows you to get rid of any valve defects (calcium deposits, growths of connective tissue).
- it may be necessary to replace the valve after 6-8 years, especially with a biological prosthesis;
- increases the risk of blood clots in the heart - blood clots;
- Open heart surgery (incision between the ribs) will take up to 1-1.5 months to recover.
Degrees of mitral valve prolapse
The word "prolapse" means "sagging". With MVP, the mitral valve leaflets are slightly stretched and this prevents them from closing tightly at the right time. In some people, MVP is a small structural feature of the heart, almost the norm, and there are no signs of illness. And others have to regularly take medication and even undergo heart surgery. Determination of the degree of mitral valve prolapse helps to prescribe the correct treatment.Degrees of prolapse
- I degree - both valves bend towards the atrium by more than 2-5 mm;
- II degree - the valves bulge by 6-8 mm;
- III degree - the sashes bend more than 9 mm.
Helps to determine the degree of MVP ultrasound procedure hearts - echocardiography. On the monitor screen, the doctor sees how much the valve leaflets bend inside the atrium, and measures the degree of deviation in millimeters. This feature underlies the division into degrees.
It is desirable that before echocardiography you did 10-20 squats. This will make violations in the heart more noticeable.
Main diagnostic criteria
- echocardiography reveals bulging of the mitral valve leaflets into the atrium;
- Doppler echocardiography determines how much blood seeps through the resulting gap back into the atrium - the volume of regurgitation.
results listening to the heart (auscultation) help to distinguish the disease from an atrial septal aneurysm or myocarditis. PMK is characterized by:
- clicks that are heard during the closing of the mitral valve;
- noises that blood creates, under pressure, breaking through a narrow gap between the valve leaflets.
mitral valve insufficiency
 Mitral insufficiency valve or mitral insufficiency - one of the acquired heart defects. With this disease, the leaflets of the mitral valve do not close completely - a gap remains between them. Each time the left ventricle contracts, some of the blood returns to the left atrium.
Mitral insufficiency valve or mitral insufficiency - one of the acquired heart defects. With this disease, the leaflets of the mitral valve do not close completely - a gap remains between them. Each time the left ventricle contracts, some of the blood returns to the left atrium. What then happens in the heart? The volume of blood in the left atrium increases, and it swells and thickens. The fibrous ring - the basis of the mitral valve, stretches and weakens. As a result, the condition of the valve gradually deteriorates. The left ventricle is also stretched, into which, after atrial contraction, too much blood enters. There is increased pressure and stagnation in the vessels going from the lungs to the heart.
Mitral valve insufficiency is the most common defect, especially in men - 10% of all acquired defects. It rarely occurs on its own, and is often associated with mitral stenosis or aortic valvular disease.
The reasons
The disease can appear during the formation of the heart during pregnancy or be the result of an illness.Congenital mitral valve insufficiency is very rare. She is called:
- underdevelopment of the left half of the heart;
- too small leaflets of the mitral valve;
- bifurcation of the valves;
- too short tendon chords that prevent the valve from closing completely.
infectious diseases
- pharyngitis
- bronchitis
- pneumonia
- periodontal disease
Autoimmune pathologies
- rheumatism
- systemic lupus erythematosus
- multiple sclerosis
These systemic diseases cause changes in the structure of the connective tissue. Cells with collagen fibers multiply rapidly. The valve leaflets shorten and look wrinkled. Compression and thickening of the petals leads to insufficiency and stenosis of the mitral valve.
Other reasons
- damage to capillary muscles after myocardial infarction;
- rupture of the valve leaflets with inflammation of the heart;
- rupture of the chords that close the valve leaflets due to a blow to the region of the heart.
Symptoms
In some people, mitral valve insufficiency does not worsen well-being and is detected incidentally. But when the disease progresses, the heart can no longer compensate for blood flow disturbances. The severity of the disease depends on two factors:- how much clearance remains between the valve leaflets at the moment of closing;
- how much blood returns to the left atrium when the ventricle contracts.
- shortness of breath on exertion and at rest;
- weakness, fast fatiguability;
- cough that gets worse when lying down
- sometimes there is blood in the sputum;
- aching and pressing pains in the region of the heart;
- swelling of the legs;
- heaviness in the abdomen under the right rib, caused by an enlarged liver;
- accumulation of fluid in the abdomen - ascites.

- bluish skin on the fingers, toes, tip of the nose (acrocyanosis);
- swelling of the neck veins;
- "heart hump" elevation to the left of the sternum;
- when tapping, the doctor notices an increase in the size of the heart;
- during probing (palpation) after squats, the doctor feels how the chest is trembling in the region of the heart. These vibrations are created by blood that passes through the hole in the valve, forming eddies and waves.
- atrial fibrillation - small non-rhythmic contractions of the atria.
- the sound from the contraction of the ventricles is weakened or not heard at all;
- you can hear the mitral valve closing;
- the most characteristic sign is the noise that is heard during systole - contractions of the ventricles. It is called "systolic murmur". It arises from the fact that blood under pressure breaks back into the atrium through loosely closed valve leaflets during ventricular contraction.
chest x-ray. The picture shows:
- enlargement of the left atrium and left ventricle;
- esophagus displaced 4-6 cm to the right;
- the right ventricle may be enlarged;
- arteries and veins in the lungs are dilated, their contours are fuzzy, blurry.
Phonocardiogram. The most informative study that allows you to study heart sounds and murmurs:
- the sound from the contraction of the ventricles is heard faintly. This is due to the fact that the ventricles almost do not close;
- murmur of blood rushing from the left stomach into the left atrium. The louder the noise, the more severe mitral insufficiency;
- an additional click is heard when the valve closes. This sound is created by the papillary muscles, valve cusps and the chords that hold them.
- an increase in the size of the left atrium;
- stretching of the left ventricle;
- incomplete closure of the valve leaflets.
Diagnostics
In order to make a diagnosis, the doctor pays attention to the characteristic signs of mitral valve insufficiency.- echocardiography- reveals the weakening of the sound from the contraction of the ventricles and the noise that creates the backflow of blood. Changes in the valve leaflets are also visible.
- Electrocardiogram shows an increase in the left atrium, left and right ventricles.
- x-ray. On the x-ray dilated vessels are visible over the entire surface of the lungs with an indistinct edge and expansion of the heart to the left.
Treatment
Mitral valve insufficiency cannot be cured with medication. There are no drugs that could restore the valve leaflets and force them to close tightly. But with the help of drugs, you can improve the functioning of the heart and unload it.- Diuretics: Indapamide It is a diuretic drug that is prescribed to rid the lungs of stagnant blood. It speeds up the production of urine and helps to remove excess water from the body. As a result, the pressure in the chambers of the heart and the vessels of the lungs decreases. Take 1 tablet in the morning. The course of treatment is 2 weeks. Your doctor may recommend taking diuretics daily long time. It must be remembered that the minerals potassium, sodium, and calcium necessary for the proper functioning of the heart are excreted in the urine. Therefore, it is necessary to take mineral supplements with the permission of the doctor.
- ACE inhibitors: Captopril Reduces the load on the heart and pressure in the vessels of the lungs, improves blood circulation. In addition, it reduces the size of the heart and allows it to more efficiently eject blood into the arteries. Helps to better carry loads. Take one hour before meals, 1 tablet 2 times a day. If necessary, after 2 weeks the dose can be doubled.
- Beta blockers: Atenolol Blocks the action of receptors that cause an acceleration of the heart rate. Reduces the impact of the sympathetic nervous system, and it is she who makes the heart contract faster. Atenolol reduces the contractility of the heart muscle, makes the heart beat smoothly, in the right rhythm and lowers blood pressure. The first week the drug is taken half an hour before meals at 25 mg / day, for the second dose it is increased to 50 mg / day, for the third week it is adjusted to 100 mg / day. It is also necessary to cancel this medicine gradually, otherwise the state of health may deteriorate sharply and myocardial infarction will occur.
- Cardiac glycosides: Digoxin Increases the concentration of sodium in the cells of the heart. Improves the conduction system of the heart, which is responsible for the rhythm of its contractions. The beats become more rare, and the pauses between them lengthen, and the heart has the opportunity to rest. Improves lung and kidney function. You need digoxin especially if mitral valve insufficiency is accompanied by atrial fibrillation. The first days of treatment should be taken at 1 mg / day. The dose is divided into 2 parts and drunk in the morning and evening. After a few days, they switch to a maintenance dose, which is 0.5 mg / day. But remember that for each person the amount of the drug is prescribed individually.
- Antiplatelet agents: Aspirin
This medicine prevents platelets and red blood cells from sticking together and forming clots. In addition, antiplatelet agents help red blood cells become more flexible and pass through the narrowest capillaries. This improves blood circulation and nutrition of all tissues and organs. Aspirin is essential for people who have an increased risk of blood clots. Take 1 time per day before meals, 100 mg / day. To reduce the risk of damage to the lining of the stomach, you can drink aspirin with meals or take the tablet with milk.
Operation types
In order to assess whether the heart needs surgery, the stage of mitral valve insufficiency is determined.Grade 1 - back reflux of blood into the left atrium is not more than 15% of the volume of blood in the left ventricle.
Grade 2 - reverse blood flow 15-30%, the left atrium is not expanded.
Grade 3 - the left atrium is moderately dilated, 50% of the blood volume from the ventricle returns to it.
Grade 4 - the reverse blood flow is more than 50%, the left atrium is enlarged, but its walls are not thicker than in other chambers of the heart.
With stage 1 mitral valve insufficiency, the operation is not performed. At 2, they can offer clipping, at stages 2 and 3, they try to perform valve plastic surgery. Stages 3-4, which are accompanied by serious changes in the valves, chords and papillary muscles, require valve replacement. The higher the stage, the greater the risk of complications and re-development illness.
clipping method
Through the artery on the thigh, with the help of a flexible cable, a special clip is delivered to the heart. This device is attached in the middle of the mitral valve. Thanks to its special design, it passes blood from the atrium to the ventricle and prevents it from moving in the opposite direction. In order to control everything that happens during the operation, the doctor uses an ultrasound probe placed in the esophagus. The procedure is under general anesthesia.
Indications for this type of operation
- stage 2 mitral insufficiency;
- reflux of blood into the left atrium reaches 30%;
- there are no serious changes in tendon chords and papillary muscles.
- allows you to reduce pressure in the left ventricle and the load on its walls;
- well tolerated at any age;
- does not require connection of a device for cardiopulmonary bypass;
- there is no need to make an incision on the chest;
- the recovery period takes several days.
- not suitable for severe valve damage.
 Modern doctors try to save the valve whenever possible: if there is no severe deformation of the valves or significant calcium deposits on them. Reconstructive mitral valve repair is performed in milder patients at any age. To correct valve defects, the doctor cuts the chest and, using a scalpel, corrects damage to the valves and aligns them. Sometimes a rigid support ring is inserted into the valve to narrow it, or the tendon chords are shortened. The operation takes place under general anesthesia and requires connection to a machine that works like an artificial heart.
Modern doctors try to save the valve whenever possible: if there is no severe deformation of the valves or significant calcium deposits on them. Reconstructive mitral valve repair is performed in milder patients at any age. To correct valve defects, the doctor cuts the chest and, using a scalpel, corrects damage to the valves and aligns them. Sometimes a rigid support ring is inserted into the valve to narrow it, or the tendon chords are shortened. The operation takes place under general anesthesia and requires connection to a machine that works like an artificial heart.
Indications for this type of operation
- 2nd and 3rd stage of mitral insufficiency
- return of blood from the left ventricle to the left atrium more than 30%;
- moderate deformation of the valve leaflets, caused by any causes.
- retains the "native" valve and improves its operation;
- less likely to have heart failure;
- lower mortality after surgery;
- fewer complications.
- not suitable for significant calcium deposition on the valve leaflets;
- cannot be done if other heart valves are affected;
- there is a risk that mitral regurgitation will recur within 10 years.
Mitral valve replacement
The surgeon removes the affected valve leaflets and puts a prosthesis in their place. Indications for this type of operation
Indications for this type of operation
- 3-4 stages of mitral valve insufficiency;
- the amount of blood that is thrown back into the atrium is 30-50% of the volume of blood in the ventricle;
- the operation is carried out even if there are no tangible symptoms of the disease, but the left ventricle is greatly enlarged and there is stagnation in the lungs;
- severe violation left ventricular functions;
- significant deposits of calcium or connective tissue on the valve petals.
- allows you to correct any violations in the valve apparatus;
- immediately after the operation, blood circulation normalizes and stagnation of blood in the lungs disappears;
- allows you to help patients with 4 degrees of mitral insufficiency, when other methods are no longer effective.
- there is a risk that the left ventricle will contract worse;
- a valve made from human or animal tissue may wear out. Its service life is about 8 years;
- silicone valves increase the risk of blood clots.
After any open heart surgery, the first day will have to be spent in intensive care and about 7-10 more days in the cardiology department. After that, another 1-1.5 months will be needed for rehabilitation at home or in a sanatorium, and you can return to normal life. It takes six months to fully restore the body. Proper nutrition, good rest and physiotherapy will allow you to fully restore health and live a long and happy life.
Mitral valve prolapse (its protrusion or incomplete closure) is a pathological condition in which there is a violation of the functions of the valve located between the ventricle and the atrium. Mitral valve prolapse, the symptoms of which may be absent in any variant in about 20-40% of cases with a predominantly accidental detection of this pathology, is characterized by very favorable prognosis in its majority, which, however, does not exclude the possibility of developing a number of very serious complications in some patients .
general description
As already noted, mitral valve prolapse often becomes an incidentally detected pathology, and in most cases it does not pose any threat to the life of patients. Nevertheless, she has characteristic features, and we will try to outline them in this article.
So, to begin with, let's dwell on what a heart valve is. As you probably know, the most appropriate analogy for the functions performed by the heart is the pump - it is the similarity with it that is noted in the work of the heart, and it is this work of the heart that ensures that blood circulates through the body properly. Opportunities for this determines the maintenance of appropriate pressure in the chambers of the heart. There are four such chambers in it, these are two atria and two ventricles. The valves of interest to us are a special type of damper, concentrated between the chambers. Due to these valves, the specified pressure is regulated, and support is provided in the movement of blood flow in the required direction.
There are four such valves, and each of them has its own characteristics and principle of operation:
- mitral valve. This valve is located between the left ventricle and the left atrium, it has two leaflets (anterior and posterior). Prolapse of the anterior leaflet of the mitral valve (that is, its protrusion) is diagnosed much more often than, respectively, prolapse of the posterior leaflet. Each of the valve leaflets has thin threads attached to them - these are chords, their attachment, in turn, is made to the papillary and papillary muscles. Ensuring the normal functionality of the mitral valve is considered with the joint work of these cusps, filaments and muscles. The contraction of the heart leads to a significant increase in pressure in it, which, in turn, ensures the opening of the valves held by the papillary muscles and chords.
- Tricuspid valve (tricuspid). This valve is located between the right ventricle and the right atrium, has three valves.
- Pulmonary valve. This valve is located between the right ventricle and the pulmonary artery, its functions are reduced, in particular, to preventing the return of blood to the right ventricle.
- aortic valve. This valve is located between the aorta and the left ventricle and ensures that blood does not return to the left ventricle.
The normal operation of the heart valves is as follows. The left ventricle has two openings. One of them refers to the left atrium (where, as we have already noted, the mitral valve is located), the other to the aorta (here, as we also noted, the aortic valve is located). Thus, the movement of blood occurs as follows: first - from the atrium through the opening mitral valve to the ventricle, then - from the ventricle through the opening aortic valve towards the aorta. The subsequent closure of the mitral valve in this process ensures that blood does not return to the atrium when the left ventricle contracts, thereby ensuring only movement towards the aorta. When the aortic valve is closed, which is produced at the moment of relaxation of the ventricle, an appropriate obstacle is provided to prevent the return of blood to the heart.
A similar principle is relevant for the functioning of the pulmonary valve and the tricuspid valve. Based on this picture, it can be understood that normal process The functioning of the valves provides a proper scheme for the movement of blood through the heart departments, and also determines the possibility of its normal circulation throughout the body.
As for the pathology of interest to us, the actual prolapse, it, as already identified initially, is a protrusion. It is formed at the moment of its closure, as a result of which the valves do not close as tightly as necessary, which means that a certain amount of blood has the opportunity to return in the opposite direction, that is, into the ventricles from the considered large vessels or into the atrium from the ventricle.
Accordingly, mitral valve prolapse at the moment at which the left ventricle contracts, leads to the fact that the blood flow occurs not only to the aorta, but also to the left atrium, where it returns back, such blood return has its own definition - regurgitation. Depending on the volume of blood returned back to the atrium, the corresponding degree of such a return, that is, the degree of regurgitation, is determined. As a rule, the pathology we are interested in, the actual mitral valve prolapse, is accompanied by an insignificant degree of this return, which, in turn, practically excludes the possibility of developing serious disorders in the work of the heart and is determined by the state within the normal range. Meanwhile, the option is not ruled out, in which the reverse flow of blood is large enough in volume, which determines the need for its correction, which may even include a possible surgical intervention for this purpose.
As for the frequency of development of such a pathology as mitral valve prolapse (MVP), the following data are available here. Thus, the frequency increases with age. Predominantly, the detection of MVP occurs in patients aged 7 to 15 years. Mitral valve prolapse in children under 10 years of age is observed with almost the same frequency in terms of gender, while in children after 10 years of age, MVP is more often diagnosed in girls - in this case, a ratio of 2: 1 is determined.
Mitral valve prolapse in newborns is extremely rare. High values of the frequency of occurrence of MVP with one or another pathology of the cardiac type in children with an actual hereditary disease for them relating to connective tissue - in this case, it is detected in approximately 10-23% of patients.
As for the adult population, here the incidence of MVP is determined on average at 5-10%. Women are predominantly affected by this pathology (up to 75%), the peak incidence is between 35 and 40 years of age.
Mitral valve prolapse can manifest itself in a primary form or in a secondary form. Primary mitral valve prolapse is the main variant of the manifestation of pathology, we will consider it in the main part of our article. As for the second form, which is secondary mitral valve prolapse, then in this case, the pathology that arose when another disease was relevant for the patient, which thus became the basis for its appearance, is considered. So, secondary prolapse develops against the background of cardiomyopathy, coronary artery disease, dysfunction of the papillary muscles, myocardial infarction or calcification of the mitral ring, as well as with systemic lupus erythematosus and congestive heart failure.
The primary form of prolapse is not only not considered as a gross pathology relevant to the heart, but is often not considered as a pathology at all. However, mycosmatous changes provoked by mitral valve prolapse, accompanied in some cases by very pronounced forms of cardiac disorders, cannot leave MVP without adequate attention, both in terms of therapeutic aspects and in terms of prognostic aspects.
Mitral valve prolapse: causes
Mostly, MVP is congenital and non-dangerous (primary), which we have already found out, as well as the result of the relevance of other pathologies in the patient. Basically, the causes of MVP are related to the fact that the violation of the structure in which this pathology is relevant is congenital, and also to the fact that the connective tissue, which forms the basis of the heart valves, is subject to weakening.
The first violation is predominantly hereditary in nature, existing in the child already at the time of his birth. As for the weakness of the connective tissue, it predominantly also has a similar (congenital) nature of occurrence. The peculiarity of PMC in this case is that, due to the weakness of the connective tissue, the valve leaflets are more easily stretched, while the chords are subject to elongation. As a result of such a picture of the processes, the closing of the valve when the blood pressure is applied is accompanied by protrusion of the valves and their loose closure.
In the vast majority of cases of congenital MVP, its course is quite favorable, is not accompanied by special symptoms and does not require serious treatment. Accordingly, in this variant, it is more expedient to define prolapse as a syndrome or feature characteristic of the body, and not as a pathology or disease.
As for secondary prolapse, it develops infrequently and certain diseases serve as a “help” for its development, this allows us to define it as an acquired prolapse. Diseases that are relevant in this case violate the structure of the chords, valves or papillary muscles, we will dwell on them in a slightly more detailed version:
- IHD, myocardial infarction. The development of MVP in myocardial infarction or coronary disease occurs in older people, the reason for this is actual circulatory disturbances, in particular concerning the papillary muscles, or it occurs due to rupture of the chords, due to which the regulation of the valve is ensured. The detection of prolapse in this case occurs, as a rule, on the basis of the appearance of severe pain in patients in the region of the heart, which is also combined with weakness and the appearance of shortness of breath.
- Rheumatism. The appearance of prolapse based on rheumatic heart disease (rheumatic heart disease) is relevant for children, in particular, it develops due to an inflammatory process that affects the connective tissue, this tissue, in turn, is the basis of the chord and valve cusps. Predominantly until the moment when MVP is detected in a child, he develops scarlet fever or tonsillitis, then (after about two weeks) an attack of rheumatism manifests itself (in which pathological conditions appear in the form of joint stiffness, pain in them, inflammation, etc.).
- Chest injury. PMK against the background of such an impact is explained by the fact that it is accompanied by a rupture of the chords. This, in turn, determines the unfavorable course for the pathology we are considering, which is particularly relevant when ignoring treatment as a necessity.
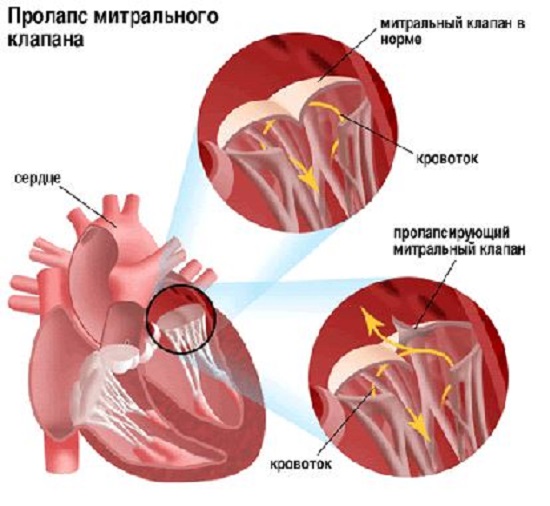
Primary mitral valve prolapse: symptoms
This variant of prolapse in patients occurs from birth. Its peculiarity lies in the fact that it can often be combined with such a disorder known to many readers as vegetative-vascular dystonia (or abbreviated VVD). All those symptoms of mitral valve collapse that a patient may experience are explained precisely by its manifestations, but they are mainly referred to as prolapse.
First of all, patients have pain in the heart and chest . Pain in the sternum with MVP is functional, respectively, this indicates that it is not a sign of any disturbances in the work of the heart, and therefore it is caused precisely by a violation of the central nervous system. Often, pain in the region of the heart occurs against the background of emotional overstrain or stress, in some cases, pain may appear at rest.
The nature of the manifestation of pain is aching or tingling, the duration of manifestation is from several seconds / minutes to several days. When trying to determine the factor that provoked the pain, it is important to take into account that pain during mitral valve prolapse in the area under consideration is not accompanied by dizziness, shortness of breath and increased pain during physical exertion. Also, pre-fainting states do not occur in this case. Otherwise, with the relevance of the listed symptoms that do not correspond to MVP, it is necessary to consult a doctor without delay - only he can reliably determine the nature pathological condition, determining whether it is a "false alarm" or indicates serious violations in the work of the heart and for the presence of serious diseases directly related to this pain.
The following symptoms, relevant for VVD and, in fact, for mitral valve prolapse, are "fading" of the heart , in "interruptions" in his work and in the increase in heart rate. The listed sensations, similarly to the symptoms listed above, are not manifestations of any pathology in the work of the heart, but only indicate increased activity central nervous system. Note also that in this case various options disturbances in the rhythm of the heart, as well as conduction, in particular, it can be ventricular and atrial extrasystole, supraventricular paroxysmal tachycardia and ventricular tachycardia, atrioventricular blockade and intraatrial blockade Ypres.
Nevertheless, as in the previous case, these states also have their deviations. In particular, they relate to the fact that palpitations with mitral valve prolapse and these manifestations, which differ from the stable work of the heart, are not manifestations of any threatening condition if they appear suddenly and disappear in the same way, without being combined with states of dizziness or loss of consciousness.
It should be noted that fainting - an extremely rare symptom for mitral valve prolapse. Its main reason lies in this case with the conditions in which a person is located or with the emotions he experiences. Fainting of this nature passes quickly enough, it is enough to change the conditions that provoke them (bring a person to his senses, provide him with access to fresh air, etc.).
Other symptoms are also characteristic of VVD, and this is an increase in temperature (up to subfebrile numbers, i.e. within 37-37.5 degrees), abdominal pain, headache, shortness of breath, a feeling of dissatisfaction with inspiration, increased fatigue and general weakness also, patients do not tolerate physical activity well. Similar to the overwhelming number of patients with a diagnosis that is relevant for them in the form of VVD, they also have meteopathy with MVP, respectively, the weather (more precisely, changes in it) often becomes the determining factor in their well-being.
As special manifestations in the picture of mitral valve prolapse, psychopathological changes are considered, in which a combination of personality and affective forms of disorders is noted. Most often affective disorders manifest in the form of depressive states, in which there is a predominance of hypochondria (an obsessive form of anxiety about one's own health, against which serious stress can develop if it is impossible to normal functioning patient) and asthenia (increased fatigue, loss or weakening of the ability in relation to the need for mental and physical stress). As for personality disorders, they may consist in the manifestation of hysteroid or sensitive traits, which in some cases leads to the development of psychopathy (pathologies of character, manifested in the form of inadequate development of volitional and emotional traits, against which the process of adapting a person to the conditions surrounding him becomes more difficult ) or to personality accentuation (an overly pronounced form of manifestation of certain traits of a person's character).
In addition to these features, patients may also show some changes associated with the skin, the functions of internal organs and the musculoskeletal system.
Often, patients with MVP also show some similarities in terms of physique. So, characteristic features in this case, there are thin and long limbs, an elongated face, high growth, a pronounced increased form of joint activity, etc.
Given the peculiarity that the connective tissue is located in the tendons, muscles and skin, the actual defect in it can cause a decrease in visual acuity in a patient, lead to the development of strabismus, and also provoke a different type of changes that will also be combined with the pathology we are considering.
Secondary mitral valve prolapse: symptoms
Secondary prolapse, as we have already discussed earlier, is acquired, it occurs against the background of transfer certain diseases patient, as well as as a result of a chest injury.
If MVP is detected after the patient suffers from scarlet fever, tonsillitis or an acute attack of rheumatic fever (with concomitant swelling, pain and redness of large joints), the likelihood of developing a rheumatic complication is considered, which, accordingly, determines rheumatic heart disease. This is accompanied by symptoms such as fatigue, dizziness, palpitations, shortness of breath (it appears after the standard type of physical exertion). In this case, the treatment of patients is carried out in a hospital. Given that inflammation of the heart valves occurs against the background of exposure to streptococcus, treatment is based on the use of antibiotics of penicillin and other groups. In addition, a treatment regimen appropriate to the patient's condition is determined.
With the development of a severe form of valve insufficiency, in which drug treatment does not help, valve replacement surgery (prosthetics) is performed.
In the presence of MVP against the background of coronary artery disease, which is particularly relevant for the elderly, a violation is considered in the form low level blood supply to the papillary muscles, which occurs when exposed to the disease, which in this case is the main one. The symptomatology in this situation consists in the appearance of pronounced attacks of pain, concentrated in the region of the heart (they can be eliminated by taking nitroglycerin), shortness of breath also appears (it is preceded by minor loads) and the previously listed forms of disturbances in the work of the heart (“fading”, “interruptions " etc.).
If the appearance of prolapse is preceded by the patient suffering an injury to the chest area, then this, as we also highlighted earlier, may be the result of rupture of the papillary muscles or chords. Here, again, symptoms in the form of "interruptions" in the work of the heart of various types, shortness of breath and weakness are relevant. The possibility of a cough is not ruled out, in which the patient has a foamy sputum of a pink hue, which necessarily requires immediate medical attention to the patient, otherwise the result of such a condition may be fatal.
Mitral valve prolapse: complications
We initially noted that, in general, mitral valve prolapse is characterized by its favorable course, in which serious complications are extremely rare. Nevertheless, they cannot be excluded, and in particular, the following pathologies are noted among them: mitral insufficiency (acute or chronic form), thromboembolism, bacterial endocarditis, arrhythmias (life-threatening), sudden death.
Mitral insufficiency develops against the background of detachment of the tendon filaments from the valve leaflets, which in this case determines the syndrome of the so-called “dangling” valve. In children, this pathology develops extremely rarely, the main cause of its occurrence is a chest injury in combination with chordate degeneration. The clinic of manifestations is reduced in this case to the sudden development of pulmonary edema. Patients develop orthopnea (which determines shortness of breath in such a variant, in which the patient is required to take a sitting position as a result of its strengthening in a horizontal position), congestive wheezing appears in the lungs, breathing becomes bubbling. Concerning chronic variant manifestations of this pathology, then it acts as an age-dependent phenomenon and develops after patients overcome the age mark of 40 years. Mitral insufficiency in 60% of cases in adults develops due to prolapse, mainly of the posterior leaflet. The nature of the manifestations is very pronounced, there are complaints about the appearance of shortness of breath during exertion, physical performance as a whole is subject to reduction, weakness and lag in terms of physical development are also relevant. The use of ultrasound makes it possible to reliably determine the degree of this kind of insufficiency, and as a method of its elimination, they are mainly guided by surgical intervention on the heart (mitral valve replacement).
Concerning arrhythmias in terms of complications of MVP, in this case they can have a very pronounced nature of manifestation, concomitant symptoms are interruptions in the work of the heart, weakness, dizziness, and sometimes short-term fainting.
An extremely serious form of complication of MVP is infective endocarditis, the frequency of its development in patients increases with age. The presence of bacteremia causes the pathogen to settle on the leaflets that have undergone changes, as a result of which the classic variant of the inflammatory process subsequently develops when bacterial vegetations form in it. Against the background of infective endocarditis, a severe form of mitral insufficiency develops, in addition, the risk of developing thromboembolism to the cerebral vessels increases, often the myocardium is involved in the process, which is also accompanied by the development of left ventricular dysfunction in patients. Among the main symptoms associated with infective endocarditis, there is a pronounced form of weakness, fever, increased heart rate, yellowness of the skin, and a decrease in pressure. Often this complication MVP develops against the background of previous dental procedures (filling, prosthetics, tooth extraction, etc.) or another type of surgical intervention. Treatment is mandatory in a hospital setting.
As for sudden death, the frequency of its occurrence in MVP is determined by the influence of many factors, among the main ones are concomitant mitral insufficiency, ventricular arrhythmia, electrical instability relevant to the myocardium, etc. In general, sudden death determines a low risk in the event that patients do not have pathology in the form of mitral regurgitation (in this case, the ratio is determined by indicators within the framework of the review of the results for the year 2 to 10,000), while its relevance increases this risk by 50 -100 times.
Diagnosis
The detection of MVP often occurs by chance, and at any age, which, as already highlighted earlier, is accompanied by an ultrasound of the heart. This method is the most effective in diagnosing mitral valve prolapse, because due to its use, the possibility of isolating a specific degree of prolapse in combination with the amount of regurgitation associated with pathology is determined.
- Mitral valve prolapse grade 1 determines the relevance for the patient of the variant of its manifestation in such a variant in which the bulging of the valves is insignificant (up to 5 millimeters).
- Mitral valve prolapse grade 2 determines the relevance of the bulging of the valves within no more than 9 millimeters.
- Mitral valve prolapse grade 3 indicates bulging of the valves from 10 millimeters or more.
It should be noted that in this version of the division of pathology into degrees, the degree of regurgitation is not taken into account, due to which now these degrees are not the basis for the subsequent determination of the prognosis for the patient and, accordingly, for the appointment of treatment. Thus, the degree of mitral valve insufficiency is determined on the basis of regurgitation, which is displayed to the greatest extent during ultrasound.
As additional diagnostic measures to determine the characteristics of the heart, an ECG procedure, as well as a Holter ECG, can be prescribed. With ECG, it is possible to study changes relevant to the work of the heart based on the impact exerted by mitral valve prolapse, while the Holter ECG allows you to record data relevant to the work of the heart within a period of 24 hours. Predominantly, the congenital form of prolapse does not disrupt the work of the heart, respectively, the need for additional measures there is no special need for diagnosing due to the practical absence of identifying certain deviations in them.
Treatment
Often, treatment of mitral valve prolapse is not necessary for patients. Its importance is considered in situations in which the heart rhythm is significantly disturbed, and heart pain also appears. The relevance of expressed forms neurotic disorders in combination with PMK may require the use of tranquilizers, methods of muscle relaxation and auto-training are considered separately.
Emphasis is also placed on the need to change lifestyle (adjustment of work / rest time, exclusion of overwork and overload (emotional, physical), as well as intoxication within the framework of production and living conditions). Balneological and climatic resorts, massage, acupuncture and water procedures are recommended. Asthenic disorders determine the need for prescribing multivitamins. Hyperventilation syndrome can be eliminated through special breathing exercises. A systematic visit to the doctor is also necessary due to the possible progression of MVP with age and the development of severe forms of complications against its background.
As part of determining the measures of drug therapy, they are guided by the treatment of VVD, psychotherapy, the prevention of the development of myocardial neurodystrophy in a patient, and the prevention of an antibacterial scale to prevent the development of complications in the form of infective endocarditis. The increase in changes in the work of the heart, as well as pronounced deflection of the valves, determines the need for surgical intervention.
What it is
Mitral valve prolapse (MVP) is a bulging, protrusion of one or both leaflets of the mitral valve of the heart (separating the left atrium from the left ventricle) into the cavity of the left atrium during the contraction of the left ventricle. It is a fairly common disease - it occurs in 15-25 percent of people. Women are 9-10 times more likely than men. It usually appears at a young age (15-30 years).
Currently, primary and secondary PMK are distinguished. The causes of primary mitral valve prolapse are heredity or congenital diseases connective tissue.
The causes of secondary MVP are rheumatism, inflammation of the heart, chest trauma and some other diseases.
How does it manifest
Most people are unaware of the presence of prolapse - their disease is asymptomatic. Possible complaints about pain in the region of the heart, usually arising against the background of emotional experiences, not associated with physical activity and not removed by nitroglycerin. Pain is usually mild, but prolonged, accompanied by anxiety and palpitations. There may be sensations of interruptions in the work of the heart.
In most cases, mitral valve prolapse proceeds favorably and does not have any effect on life and work capacity.
Diagnosis
Mitral valve prolapse sometimes causes a soft systolic murmur heard on auscultation (listening) over the apex of the heart and in the projection of the mitral valve. But more often, the presence of MVP is detected by chance during echocardiography. This method also allows you to identify the degree of prolapse and its effect on normal blood flow.
Treatment
With a low degree of mitral valve prolapse and the absence of rhythm disturbances, active treatment is not required. With severe prolapse, accompanied by pain, rhythm disturbances, beta-blockers are used. In exclusively rare cases surgical treatment is required.
The method of treatment is chosen depending on the degree of mitral valve prolapse and its effect on blood flow. The condition is monitored by echocardiography, which is carried out, as a rule, once a year.
mitral valve prolapse
Mitral valve prolapse is one of the congenital features of the structure of the heart. To make it easier to understand what exactly this feature consists of, let's briefly consider some of the nuances of the anatomy and physiology of the heart.
So, the heart is a muscular organ, the function of which is to pump blood around the body. The heart consists of two atria and two ventricles. Between the atria and ventricles are the valves of the heart, tricuspid (tricuspid) on the right and mitral (bicuspid) on the left. The valves are made of connective tissue and look like a kind of doors that close the holes between the atria and ventricles so that the blood moves in the right direction - normally, blood moves from the atria to the ventricles, there should not be a back throw into the atria. At the moment of expulsion of blood from the atrium into the ventricle (atrial systole), the valve is open, but as soon as all the blood has entered the ventricle, the valve leaflets close, and then the blood is expelled from the ventricles into the pulmonary artery and aorta (ventricular systole).

From left to right: 1. General diastole of the heart - the atria and ventricles are relaxed; 2. Atrial systole - the atria are contracted, the ventricles are relaxed; 3. Ventricular systole - the atria are relaxed, the ventricles are contracted.
If the leaflets of the mitral valve do not completely close during the period of expulsion of blood from the ventricle to the aorta, then they speak of its prolapse (sagging) into the cavity of the left atrium at the time of systole (contraction of the left ventricle).
Mitral valve prolapse- this is a violation of its connective tissue structure, leading to incomplete closure of the valves, as a result of which blood may be thrown back into the atrium (regurgitation). Distinguish between congenital (primary) and developed against the background of endocarditis, myocarditis, chest trauma with chord rupture, heart defects, myocardial infarction (secondary) prolapse. Primary prolapse occurs in approximately 20-40% of healthy people and in most cases does not cause significant influence on the function of the cardiovascular system.
In modern medicine, primary mitral valve prolapse is considered to be rather congenital feature structure of the heart, rather than a serious pathology, provided that it is not combined with gross malformations and does not cause significant hemodynamic disturbances (functions of the cardiovascular system).
Causes of mitral valve prolapse
Below we will talk about primary mitral valve prolapse, which refers to small anomalies in the development of the heart. What could be causing this anomaly? The main reason for the development of the disease is a genetically determined violation of the synthesis of type 111 collagen. This is a protein that takes part in the formation of connective tissue in all organs, including the heart. If its formation is disturbed, the connective tissue “skeleton” of the valve loses its strength, the valve becomes looser, softer, and therefore cannot provide sufficient resistance to blood pressure in the cavity of the left ventricle, which leads to sagging of its valves into the left atrium.
It is also necessary to take into account harmful factors that affect the development of the fetus and connective tissue during pregnancy - smoking, alcohol, narcotic and toxic substances, occupational hazards, poor nutrition, stress.
Symptoms and signs of mitral valve prolapse
As a rule, the diagnosis is established during a routine examination of newborns, including the method of echocardiography (ultrasound of the heart).
 Mitral valve prolapse is classified according to the degree of regurgitation (reverse reflux of blood) determined by Doppler ultrasound of the heart. The following degrees are distinguished:
Mitral valve prolapse is classified according to the degree of regurgitation (reverse reflux of blood) determined by Doppler ultrasound of the heart. The following degrees are distinguished:
— 1 degree- the reverse flow of blood in the left atrium remains at the level of the valve cusps;
— 2 degree- the blood stream returns to half of the atrium;
— 3 degree- the reverse reflux of blood fills the entire atrium.
If the patient has congenital prolapse, then as a rule, regurgitation is insignificant (grade 1), or it is not at all. If valve prolapse is secondary, then hemodynamically significant regurgitation may develop, since the return of blood to the atrium has a negative effect on the functions of the heart and lungs.
With prolapse without regurgitation, there are no clinical symptoms. Like other small anomalies of the development of the heart ( additional chord. an open oval window), this disease can be suspected only on the basis of a routine examination of the child and an ECHO-KG, which in recent years has been a mandatory method for examining all children aged 1 month.
If the disease is accompanied by regurgitation, then with psycho-emotional or physical stress, there may be complaints of diffuse pain in the region of the heart, sensations of interruptions in the work of the heart, a feeling of "fading" of the heart, shortness of breath, a feeling of lack of air. Since the activity of the heart and the autonomic nervous system (the part of the nervous system responsible for the functions of internal organs) is inextricably linked, the patient may be disturbed by dizziness, fainting, nausea, "lump in the throat", fatigue, unmotivated weakness, excessive sweating, tachycardia (rapid heartbeat), a slight increase in temperature. All these are symptoms of vegetative crises, which are especially pronounced in a child with prolapse during adolescence, when there is rapid growth and hormonal changes in the body.
In rare cases, when grade 3 regurgitation is observed, the above complaints are accompanied by manifestations characteristic of hemodynamic disorders in the work of the heart and lungs - pain in the heart and shortness of breath during normal household activity, walking, climbing stairs, due to stagnation of blood in these organs. Also rarely, cardiac arrhythmias can join - sinus tachycardia, atrial fibrillation and flutter, atrial and ventricular extrasystoles, short PQ syndrome. It must be remembered that sometimes regurgitation can progress, that is, the degree of prolapse increases.
Diagnosis of mitral valve prolapse
What is the diagnosis based on? Mitral valve prolapse can be suspected even during the clinical examination of the child. In young children, prolapse may be accompanied by umbilical and inguinal hernia, hip dysplasia (congenital subluxation and dislocation of the hip). When examining children and adolescents, the appearance of the patient draws attention - tall, long fingers, long limbs, pathological joint mobility, curvature of the spine, deformity of the chest.
During auscultation (listening), either isolated systolic murmurs and clicks are heard (due to the tension of the tendon chords when the valve prolapses at the time of its closure), or a combination of them.
The main diagnostic method is echocardiography (ultrasound of the heart) with Doppler study(allows you to display an echo - a signal from moving blood structures). Direct ultrasound allows you to assess the presence of valve prolapse and the degree of its sagging, and the Doppler detects the presence and degree of regurgitation.
In addition, an ECG and daily ECG monitoring are required to determine rhythm and conduction disturbances (cardiac arrhythmias).
X-rays of organs are also shown chest cavity to determine whether the shadow of the heart is expanded in diameter and whether there is stagnation of blood in the vessels of the lungs, which may indicate the development of heart failure.
If necessary, tests with a load are prescribed (treadmill test - walking on a treadmill, bicycle ergometry).
Mitral valve prolapse treatment
In the event that mitral valve prolapse is not accompanied by the presence of clinical symptoms, the patient is not prescribed drug therapy. There is also no need for hospitalization. The implementation of a number of restorative measures and observation by a cardiologist with an annual ECHO-KG are shown.
General strengthening measures include: good nutrition, a rational regime of work and rest with sufficient sleep, walks in the fresh air, general hardening of the body, moderate exercise (permitted by a doctor).
With manifestations of vegetative - vascular dystonia (vegetative crises), spinal massage, physiotherapy exercises, electrophoresis with magnesium preparations on the collar zone are prescribed. Herbal sedative preparations (motherwort, valerian, sage, hawthorn, rosemary), as well as drugs that improve the nutrition of the heart muscle (magnerot, carnitine, riboxin, panangin) and vitamins are shown.
With pronounced sensations of interruptions in the heart, and even more so with rhythm disturbances confirmed by ECG, adrenoblockers are prescribed (carvedilol, bisoprolol, atenolol, anaprilin, etc.)
In rare cases (with the development of heart failure, arrhythmias, progressive mitral valve insufficiency), surgical correction prolapse. Surgical treatments include recovery operations on the valve (suturing its sagging leaflet, shortening the stretched chord) or prosthetic valve replacement with an artificial one. Surgery isolated congenital prolapse is used extremely rarely due to the favorable course of this pathology.
Complications of mitral valve prolapse
Are complications possible? Despite the fact that in most cases mitral valve prolapse occurs with minor regurgitation, which does not require special therapy, there is still a risk of complications. Complications are quite rare (only 2-4%) and include the following life-threatening conditions that require treatment in a specialized hospital:
— acute mitral insufficiency- a condition that usually occurs as a result of the detachment of tendon chords in case of chest injuries. It is characterized by the formation of a “dangling” valve, that is, the valve is not held by the chords, and its valves are in free movement without performing their functions. Clinically, a picture of pulmonary edema appears - severe shortness of breath at rest, especially when lying down; forced sitting position (orthopnea), bubbling breathing; congestive rales in the lungs.
— bacterial endocarditis- a disease in which microorganisms settle on the inner wall of the heart, breaking into the blood from the source of infection in the human body. Most often, endocarditis with damage to the heart valves develops after tonsillitis in children, and the presence of initially altered valves can serve as an additional factor in the development of this disease. Two to three weeks after the infection, the patient develops a recurrent fever, chills, there may be a rash, an enlarged spleen, cyanosis (blue coloration of the skin). it serious disease, which leads to the development of heart defects, gross deformation of the heart valves with impaired functions of the cardiovascular system. Prevention of bacterial endocarditis is the timely sanitation of acute and chronic foci of infection ( carious teeth, diseases of ENT - organs - adenoids, chronic inflammation of the tonsils), as well as prophylactic antibiotics for procedures such as tooth extraction, removal of the tonsils.
— sudden cardiac death- a formidable complication, characterized, apparently, by the occurrence of idiopathic (sudden, causeless) ventricular fibrillation, which refers to fatal arrhythmias.
Prognosis for mitral valve prolapse
The prognosis for life is favorable. Complications rarely develop, and the patient's quality of life does not suffer. However, the patient is contraindicated in certain sports (jumping, karate), as well as professions that cause an overload of the cardiovascular system (divers, pilots).
Regarding military service, it can be said that, according to orders, fitness for military service is decided individually for each patient at the military medical commission. So, if a young man has mitral valve prolapse without regurgitation or with regurgitation of the 1st degree, then the patient is fit for service. If there is regurgitation of the 2nd degree, then the patient is conditionally fit (he will not be called up in peacetime). In the presence of regurgitation of the 3rd degree, rhythm disturbances or heart failure of a functional class of 11 and above, military service is contraindicated. Thus, most often a patient with mitral valve prolapse with a favorable course and in the absence of complications can serve in the army.
Therapist Sazykina O.Yu.
Mitral valve prolapse. Heart disease. Diagnosis of prolapse
Mitral valve prolapse- symptoms and detection of the disease.
One of the heart defects is called mitral valve prolapse in medicine.. Behind this terrible name lies an equally terrible disease. And, like many heart diseases, mitral valve prolapse may not make itself felt for several years. O terrible diagnosis the patient learns only at the appointment with the cardiologist according to the results of the performed electrocardiography (ECG) and blood tests.
What is this disease? mitral valve prolapse
 The human heart is made up of four chambers - two ventricles and two atria.. During atrial contraction, the mitral valve (the septum between the left atrium and the left ventricle) lets blood into the ventricle. Normally, after that, it closes tightly, but with prolapse, the valve bends, which causes a small amount of blood to flow back into the atrium. In some cases, the amount of blood outflow is so high that the patient needs surgical correction of the defect.
The human heart is made up of four chambers - two ventricles and two atria.. During atrial contraction, the mitral valve (the septum between the left atrium and the left ventricle) lets blood into the ventricle. Normally, after that, it closes tightly, but with prolapse, the valve bends, which causes a small amount of blood to flow back into the atrium. In some cases, the amount of blood outflow is so high that the patient needs surgical correction of the defect.
The development of mitral valve prolapse disease is most susceptible to women aged fourteen to thirty years. Cardiologists still cannot say for sure what exactly is the cause of this heart disease. .
The symptoms accompanying the disease are similar in the manifestation of other heart diseases:
- sharp or aching pains in the left side of the chest, which are not subject to relief with traditional medicines and are not associated with great physical exertion, are usually observed in the morning or at night,
- a feeling of lack of air, it is impossible to take a deep breath,
- feeling of rapid heartbeat,
- pre-consciousness (ringing in the ears, darkening of the eyes, dizziness, loss of consciousness),
- rare slight increase in temperature.
 There are two main methods instrumental diagnostics. which allow you to accurately diagnose mitral valve prolapse - ECG and echocardiography. To control the state of health of their body, cardiologists of the medical center "Your Doctor" recommend that patients undergo an examination at medical professionals at least once a year. With a regular manifestation of the disease in the form of pain, rhythm and heart disturbances, a course of active drug treatment may be necessary. Most of the treatment can be done under the supervision of doctors in the day hospital of the medical center "Your Doctor". In rare protracted cases, it may be necessary to perform plasty and valve prosthetics.
There are two main methods instrumental diagnostics. which allow you to accurately diagnose mitral valve prolapse - ECG and echocardiography. To control the state of health of their body, cardiologists of the medical center "Your Doctor" recommend that patients undergo an examination at medical professionals at least once a year. With a regular manifestation of the disease in the form of pain, rhythm and heart disturbances, a course of active drug treatment may be necessary. Most of the treatment can be done under the supervision of doctors in the day hospital of the medical center "Your Doctor". In rare protracted cases, it may be necessary to perform plasty and valve prosthetics.
Mitral valve prolapse is the sagging of one or both leaflets of the mitral valve into the cavity of the left atrium during systole - contraction of the ventricles of the heart. The mitral valve is a formation located between the left atrium and the left ventricle and consisting of a valve ring, two leaflets and a subvalvular apparatus supporting the leaflets - chords and papillary muscles. During systole (contraction), the atrial valve is open and blood flows freely into the ventricle. Then it closes, and during ventricular systole, when blood is sent to the aorta, it prevents the reverse flow of blood - regurgitation - from the ventricle to the atrium. Normally, the leaflets of the mitral valve should close completely. If this does not happen, then some of the blood is thrown into the left atrium.
A doctor can suspect mitral valve prolapse by listening with a phonendoscope in a patient, usually a child or young person, systolic murmur. This murmur differs in its characteristics from the murmurs heard with heart defects, it is softer and more unstable, but, nevertheless, before, when there was no echocardiography, such patients were often diagnosed with rheumatism with damage to the heart valves.
Prolapse is a serious disease that can lead to complications.- the appearance of fainting, heart rhythm disturbances, the formation of blood clots on the altered valve, which can lead to the development of ischemic stroke at a young age. Changes in the structure of the valve also lead to an increased risk of infection with the development of infective endocarditis, so these patients need antibiotic prophylaxis before any upcoming surgery and even tooth extraction.
Causes and manifestations.
Mitral valve prolapse can be primary (idiopathic) or secondary. Secondary prolapse is a manifestation of various diseases leading to the destruction of the valves, rupture of chords and papillary muscles: coronary heart disease, myocardial infarction, defects, inflammatory and degenerative diseases.
The causes of primary, or idiopathic, prolapse can be- hereditary weakness of the connective tissue (the tissue that makes up the heart valves, as well as ligaments, tendons, supporting apparatus of various organs, components of the vascular wall, etc.). These patients usually have other manifestations of this congenital anomaly.
prolapse treatment.
Prolapse mild degree, that is, less than 10 mm, does not require special treatment. It is detected, as a rule, in childhood and young age, and then, with an increase in the density of the connective tissue, it may disappear. Treatment may require the above comorbid conditions associated with weakness of the connective tissue. To improve its structure, as well as to normalize the functional state of the cardiovascular system, potassium, magnesium, copper, vitamins and other drugs are often prescribed, depending on numerous symptoms.
With severe prolapse, sports are contraindicated, since dizziness and fainting in patients can no longer occur due to improper redistribution of vascular tone, but due to the low ejection syndrome associated with the fact that significant regurgitation occurs during intense physical exertion, and most of blood from the left ventricle does not go to the aorta, but returns to the cavity of the left atrium.
Due to the risk of thrombus formation on the myxomatous valve, to prevent ischemic stroke, such patients may require special antithrombotic therapy. They are also advised to prescribe prophylactic antibiotics well in advance of any surgery and dental procedures. Sometimes surgical treatment is necessary to correct severe prolapse.
Complications of mitral valve prolapse include mitral regurgitation, infective endocarditis, atrial fibrillation. Visit the cardiologist and other doctors of the medical center "Your Doctor" in a timely manner. In this case, complications can be avoided .



