Bacterial vaginosis causes ways of infection. Bacterial vaginosis: treatment - schemes. What is meant by bacterial vaginosis
Bacterial vaginosis- symptoms and treatment
What is bacterial vaginosis? We will analyze the causes of occurrence, diagnosis and treatment methods in the article by Dr. Yu.A. Chursina, a gynecologist with an experience of 6 years.
Definition of illness. Causes of the disease
Bacterial vaginosis- This is an infectious non-inflammatory disease in which an abundant growth of certain microorganisms occurs in the vagina and a sharp decrease in lactic acid bacteria with protective properties.
This pathology is one of the most common diseases of the female genital area. According to various estimates, it is found in approximately 70% of women of reproductive age.
Let's take a look at the name of the disease. The term "bacterial" emphasizes a significant increase in the number of aerobic and especially anaerobic bacteria that obtain energy from a minimum amount of oxygen. The meaning of the word "vaginosis" indicates that there are no signs of inflammation in this disease.
Previously, it was mistakenly called "gardnerellosis", since it was believed that bacteria were the cause of the pathology. Gardnerella vaginalis. However, it was found that these microorganisms are found not only in patients with symptoms of the disease, but also in 40% of women who do not have complaints. Therefore, the diagnosis of Gardnerellosis is incorrect and incorrect: it does not reflect either the etiology or pathogenesis of the disease, and in some cases leads to a false positive diagnosis and the appointment of unreasonable treatment.
The causes of bacterial vaginosis are very diverse. These include both banal violations of intimate hygiene, and more complex situations.
Factors contributing to the onset of the disease include:
- trauma during childbirth;
- various operations on the perineum;
- surgical abortion;
- menstrual irregularities;
- irrational use of antibiotics and even local antiseptics.
If you experience similar symptoms, consult your doctor. Do not self-medicate - it is dangerous for your health!
Symptoms of bacterial vaginosis
The main symptom of bacterial vaginosis is a copious liquid homogeneous discharge from the genital tract with an unpleasant odor. They can be gray or white.

The smell of secretions is often compared to the smell of fish. It is especially strongly felt when the vaginal environment is alkalized - after intercourse and during menstruation.
Approximately 50% of women, that is, every second woman, have no complaints about vaginal discharge, so the disease may be asymptomatic.
Sometimes with bacterial vaginosis, patients are concerned about discomfort, itching or burning in the vagina and in the rectal area, urination disorders and pain during or after intercourse.
A burning sensation and itching are also characteristic of vaginitis, an inflammatory process in the vagina. It is distinguished from bacterial vaginosis by a feeling of vaginal dryness, as well as redness and swelling of its membrane.
The pathogenesis of bacterial vaginosis
Bacterial vaginosis does not have one specific pathogen - it can be caused by various microorganisms. The most frequent include not only the mentioned G.vaginalis, but also fusobacteria, peptostreptococci, veillonella, vaginal atopobium, as well as bacteria Peptoniphilus, Prevotella, P. bivia And M. mulieris. Most often, the development of the disease provokes a combination of 2-3 microorganisms or more.
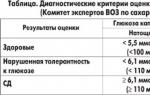
In the presence of risk factors, these pathogens begin to actively multiply in the course of their life, alkalizing the vaginal environment (normally, the pH of vaginal discharge is 3.5-4.5). Only lactobacilli that secrete lactic acid can prevent the growth of pathogenic bacteria, but due to an increase in the pH of the medium, their number decreases.
According to modern ideas, the bacteria that cause bacterial vaginosis are able to create biofilms that attach to the vaginal epithelium. Inside these films, microorganisms become less vulnerable to exposure, including drugs. It is the formation of biofilms that is the cause of frequent recurrence and unsuccessful treatment of the disease.
Bacterial vaginosis is not a sexually transmitted disease, as it also occurs in girls who have never had sex. Although it is difficult to unequivocally state that the disease is not related to its sexual transmission: numerous studies confirm that the change of sexual partner, the presence of numerous sexual partners, as well as non-traditional sex significantly increase the number of relapses of bacterial vaginosis.
Classification and stages of development of bacterial vaginosis
At the moment, there is no classification and division into stages of the disease. There is also no code in the ICD-10 (International Classification of Diseases) that would correspond to the diagnosis of "Bacterial vaginosis". Other codes are used to encode this state. Most often it is referred to as "N86. Other inflammatory diseases of the vagina", which is incorrect and not always correct.
Previously, the classification proposed by E.F. Kira in 1995. According to her, four types of vaginal microbiocenosis were distinguished - a combination of microorganisms that live in the vagina:
- Normocenosis - the predominance of lactobacilli. is a sign of the normal microflora of the vagina.
- Intermediate type - a moderate or reduced number of lactobacilli, the presence of gram-positive cocci and gram-negative rods. Often observed in healthy women, it can rarely be accompanied by complaints of discharge from the genital tract.
- Dysbiosis - almost complete absence of lactobacilli, abundant polymorphic gram-negative and gram-positive rod and coccal microflora. This condition has been associated with bacterial vaginosis.
- Vaginitis - an increase in the number of leukocytes in smears. This condition has been associated with nonspecific vaginitis.
Today, this classification is not used due to a significant expansion of knowledge about the microbiocenosis of the vagina and the emergence of modern methods of laboratory diagnostics.
Complications of bacterial vaginosis
Unpleasant discharge from the genital tract significantly reduces a woman's quality of life and her self-esteem, causes sexual behavior disorders, and can even lead to.
In general, bacterial vaginosis can cause a number of fairly serious complications. Scientists have proven the impact of the disease on the course of pregnancy: it doubles the risk of preterm birth, especially if it is detected at the beginning of the second trimester. Complications can also occur after the birth of a child: postpartum endometritis, wound infection after a cesarean section. Some researchers suggest that the toxins of vaginosis pathogens can affect the fetus, penetrating the placenta, which in the future may become one of the causes of the child.
More recently, bacterial vaginosis has also been shown to be associated with: in patients with this non-inflammatory disease of the vagina, the risk of infection with the human papillomavirus is higher than in healthy women. It also speaks to an increased risk of cervical neoplasia.
In addition, at the moment, the possible relationship of bacterial vaginosis with an increased risk of infection and other sexually transmitted diseases is being actively discussed (,). In particular, one study noted that an HIV-infected woman with bacterial vaginosis was more likely to transmit HIV to a sexual partner than an HIV-infected woman without vaginosis.
Diagnosis of bacterial vaginosis
Diagnosis of bacterial vaginosis usually does not present significant difficulties. Nevertheless, when making a diagnosis, one can often encounter errors: both overdiagnosis (when a patient is attributed a disease that she does not actually have), and underdiagnosis.
Most often, it is possible to correctly determine the disease already at the first visit of a woman to a doctor. In such cases, the diagnosis is made on the basis of characteristic complaints, examination data and pH-metry of vaginal discharge. Sometimes a fairly extensive clinical and laboratory examination may be required.
R. Amsel criteria are used in the diagnosis of bacterial vaginosis. These include:
- the presence of homogeneous whitish-gray discharge from the genital tract (on examination, one can note their uniform distribution along the walls of the vagina);
- increase in Ph in the vagina - more than 4.5;
- positive test with 10% potassium hydroxide solution - determination of volatile amines;
- detection in native smears and / or in Gram smears of "key cells", i.e. cells of the vaginal epithelium with gram-variable microorganisms tightly attached to their surface. Leukocytes in these smears are not detected or are contained within the normal range, which indicates the absence of inflammation, and lactobacilli are reduced to the point of complete absence.

The diagnosis of "Bacterial vaginosis" is established in the presence of at least three signs.
There is also a semi-quantitative assessment of smears of vaginal fluid, Gram-stained, on a scale of 0 to 10. Now this method is practically not used.
For laboratory diagnosis of bacterial vaginosis, the PCR Real Time method is used as part of a comprehensive analysis of the vaginal microflora. There are a number of test systems, the most common of which are Femoflor 16+KVM and Femoflor screen. These test systems allow you to get a fairly complete picture of the characteristics of the microbiocenosis of the woman's vagina and prescribe a reasonable treatment.
Clinical diagnostic methods include various rapid tests: Fem-exam, BVBlue, Pip-activity TestCard. However, all of them are not widely used in clinical practice. This is mainly due to their lack of sensitivity.
In addition, it must be remembered that any woman who is sexually active and goes to the doctor with complaints of discharge from the genital tract must be screened for causative agents of trichomoniasis, gonorrhea, due to the wide spread of these infections and the high frequency of complications.
Treatment of bacterial vaginosis
In no case should you self-medicate - it must be prescribed by a doctor, otherwise it may adversely affect the woman's health.
Treatment of bacterial vaginosis is carried out in the presence of clinical and laboratory signs. Pregnant women deserve special attention. Discussions about the advisability of their treatment have already been closed: it is mandatory for all pregnant patients, including those with a low risk of preterm birth (cases where there were no preterm births in the past). Treatment of pregnant women with asymptomatic bacterial vaginosis and a high risk of preterm birth (if children were already born before the due date) can significantly reduce the risk of early termination of pregnancy.
To eliminate bacterial vaginosis, antiseptic agents and various combined preparations are used. At present, the effectiveness of a two-stage treatment regimen has been proven: the first stage consists in the use of antiseptic agents, and the second - in the restoration of the vaginal microflora.
There are quite a lot of both foreign and Russian recommendations and treatment regimens for this disease. In accordance with the Eurasian clinical guidelines for the rational use of antimicrobial agents in outpatient practice, the following drugs should be used when eliminating bacterial vaginosis:
First line therapies:
- cream "Clindamycin" 2%;
- gel "Metronidazole" 0.75%;
- "Metronidazole" 0.5 g (for oral administration);
- "Ornidazole" 0.5 g (for oral administration).
Second line therapies:
- candles "Clindamycin" 0.1 g;
- "Clindamycin" 0.3 g (for oral administration);
- "Metronidazole" 2.0 g (for oral administration).
The duration and frequency of taking these drugs is determined by the doctor individually. In addition, there are a significant number of combined drugs.
To restore the vaginal microflora, vaginal capsules with live lactobacilli, ascorbic acid for vaginal use, and lactic acid gel can be used.
A promising method for the treatment of bacterial vaginosis at the moment is the treatment of the vagina with ultrasound-cavitated antiseptic solutions. This method is being actively studied and great hopes are placed on it in the treatment of not only bacterial vaginosis, but also various inflammatory diseases of the skin and mucous membranes.
Forecast. Prevention
The prognosis for timely treatment is favorable in most cases. Sometimes relapses of the disease are possible. When they occur, a comprehensive approach to the patient is required, a complete clinical and laboratory examination and the exclusion of concomitant diseases that may increase the risk of recurrence of bacterial vaginosis. You also need to consult on nutrition and lifestyle issues.
As a preventive measure for the occurrence of bacterial vaginosis, first of all, it is necessary to exclude such risk factors as:
- violation of the integrity and anatomy of the external genital organs of a woman (may occur with injuries during childbirth, various surgical interventions);
- alkalization of the vaginal environment (possible with the use of certain lubricants, shower gels, douching);
- surgical abortions, some gynecological operations, accompanied by the removal of the mucous plug from the cervical canal;
- menstrual disorders, hypoestrogenic state in the period before menopause;
- irrational use of antimicrobial agents and antiseptics.
A significant contribution to the development and recurrence of the disease is made by frequent changes of sexual partners, severe concomitant diseases, alcohol abuse, and smoking. All this should be avoided.
An important role in prevention is played by a healthy lifestyle, adequate physical activity and adherence to proper nutrition - a vegetarian diet and increased consumption of "fast" carbohydrates increase the risk of relapse.
To prevent bacterial vaginosis, you need to follow the recommendations for intimate hygiene:
- Wash at least twice a day. To wash the genitals, use only warm water or special compositions for intimate hygiene, which contain substances that do not violate the acidity of the vaginal environment.
- Washing should only be done with cleanly washed hands, do not use washcloths. When washing, the water jet should be directed from front to back.
- After washing, it is necessary to blot moisture with a towel for intimate hygiene. It should be soft, clean and strictly individual. You can not use them for hands, face and other parts of the body.
- During menstruation, it is not recommended to take a bath, swim in the pool or ponds. It is preferable to take a shower in the morning and in the evening. It is better to avoid sexual intercourse, especially in the first days of menstruation.
- Sanitary pads during menstruation must be changed at least four to five times a day, tampons - every two hours.
- Daily sanitary napkins should not be used regularly.
- Do not apply vaginal douching for regular hygiene. They are possible only if they are prescribed by a doctor.
- Give preference to underwear made of natural fabrics with a wide gusset. It should be changed daily, in some cases twice a day. Wash underwear separately from other clothes, towels and bed linen.
Bacterial vaginosis- a disease with characteristic abundant and prolonged discharge from the vagina, often with an unpleasant odor. They do not detect gonococci, Trichomonas and fungi. The use of the term "bacterial" is due to the fact that the disease is caused by polymicrobial microflora; vaginosis - since, unlike vaginitis, there are no signs of an inflammatory reaction of the vaginal mucosa.
SYNONYMS OF BACTERIAL VAGINOSIS
Nonspecific vaginosis, anaerobic vaginosis, vaginal bacteriosis, vaginal lactobacillosis, aminocolpitis, gardnerellosis, mobiluncosis, vaginal discharge with key cells, "lactobacterium deficiency syndrome" and etc.
ICD-10 CODE In ICD-10, this disease is not registered, since the term " bacterial vaginosis” arose after the publication of this classification.
EPIDEMIOLOGY OF BACTERIAL VAGINOSIS
Bacterial vaginosis- the most common infectious disease of the female reproductive system. The prevalence of bacterial vaginosis in different populations of women and in different countries ranges from 15 to 80% or more. According to official medical statistics in Western countries, the symptoms of vaginosis, mainly discharge, are found annually in more than 10 million women. Bacterial vaginosis is common with equal frequency among women of different racial groups. Data on the incidence of bacterial vaginosis is variable, which is due to different populations of examined women, the use of non-standard diagnostic methods, an ambiguous interpretation of the disease, and ignoring social and demographic factors.
Bacterial vaginosis is not sexually transmitted. However, it has been established that there is a certain correlation between the occurrence of bacterial vaginosis and sexual behavior: the early onset of sexual activity, its characteristics, the number of sexual partners, etc. The number of sexual partners is a more significant factor for the development of bacterial vaginosis than the number of sexual contacts. Sexual activity in bacterial vaginosis is higher than in the group of healthy women.
PREVENTION OF BACTERIAL VAGINOSIS
For the prevention of bacterial vaginosis, it is necessary to normalize the hormonal status, limit the intake of broad-spectrum antibiotics, maintain personal hygiene, exclude promiscuity, timely treatment of sexually transmitted diseases and intestinal dysbacteriosis. An important aspect of the problem of dysbiotic diseases of the vagina, bacterial vaginosis is preventive measures, such as sex education, training in the proper use of contraceptives and antibacterial drugs.
SCREENING
All patients with complaints of leucorrhea with an unpleasant odor, itching, burning in the vagina and perineum, dyspareunia are subject to examination. All pregnant women are subject to mandatory examination during the initial visit to the antenatal clinic, as well as in each trimester and before childbirth.
CLASSIFICATION OF BACTERIAL VAGINOSIS
There are currently several classifications of vaginal dysbiosis taken for classification of bacterial vaginosis(Table 20-4).
Table 20-4. Classification of vaginal dysbacteriosis (VDD)
| Author | Year | Principle of classification | Type of biocenosis |
| Kira E.F. | 1995 | Type of microbiocenosis of the vagina | - normocenosis - intermediate - dysbiosis (vaginosis) - vaginitis |
| Zhukova G.I. Ankirskaya A.S. | 1992-1995 | Clinical course of DBP | - acute - torpid - asymptomatic |
| Bayramova G.R. | 1996 | Clinical course of DBP | - asymptomatic with a clinical picture - monosymptomatic - polysymptomatic |
| Taylor–Robinson D., Hay P.E. | 1997 | Clinical course of DBP | - temporary - intermittent - persistent |
| Mavzyutov A.R. et al. | 1998 | Severity of ABP | I degree - compensated II degree - subcompensated III degree - decompensated |
As can be seen from the table, most classifications reflect certain aspects of the clinical course of bacterial vaginosis. So, if the clinical classifications of Zhukova G.I. (1992), Ankirskaya A.S. (1995) and Bayramova G.R. (1996) are very similar and almost identical, then the classification of Mavzyutov A.R. et al. (1998) reflects the severity of PAD. according to this classification.
- I degree of severity (compensated WBP):
- complete absence of microflora in the material;
- unchanged epitheliocytes;
- the possibility of settling an ecological niche with microorganisms entering from outside. - II degree (subcompensated DBA):
- quantitative reduction of lactobacilli;
- increase in gram-variable bacterial microflora;
- 1-5 "key" cells in the field of view, moderate leukocytosis 15-25 in the field of view. - III degree (decompensated DBP):
- severe clinical symptoms of bacterial vaginosis;
- complete absence of lactobacilli;
- the entire field of vision is filled with QC;
- microflora - various microorganisms in different morphological and species combinations, except for lactobacilli.
Reasons for the development of bacterial vaginosis I degree of severity:
excessive preparation of the patient for a visit to the doctor, improper sampling of material, intensive chemotherapy with broad-spectrum antibacterial drugs.
Dermatovenereologists (Yu.K. Skripkin), by analogy with venereal diseases, distinguish three phases of bacterial vaginosis: fresh, torpid and chronic bacterial vaginosis with an incubation period of 5 days to 3 weeks. In the acute period, hyperemia of the mucous membrane of the cervix and vagina is possible. However, it should be noted that none of the existing classifications is indisputable. This highlights the need for further clinical and laboratory research on bacterial vaginosis.
ETIOLOGY (CAUSES) OF BACTERIAL VAGINOSIS
It is generally accepted that there are no specific causative agents of bacterial vaginosis. In the role of the etiological factor of bacterial vaginosis is the association of anaerobic and facultative anaerobic microorganisms. Among the microorganisms associated with bacterial vaginosis, Mobiluncus spp., Bacteroides spp., peptococci, peptostreptococci, etc. are more common. Gardnerella and mycoplasmas are also found in polymicrobial complexes. For such polymicrobial processes (mixed infections), it is characteristic that the etiological factor is not one of any microorganism, but their association with its inherent biological properties. An important circumstance is that against the background of a sharp decrease or complete disappearance of lactic acid bacteria, primarily lactobacilli that produce hydrogen peroxide, in quantitative terms, the total vaginal contamination increases to 1010 CFU / ml of vaginal fluid. The share of strict non-spore-forming anaerobic microorganisms mainly increases.
PATHOGENESIS OF BACTERIAL VAGINOSIS
Explaining the violations of the microecology of the vagina and the development of a characteristic symptom complex of bacterial vaginosis is one of the complex issues of the pathogenesis of the ongoing processes. The disappearance of lactomicroflora and excessive growth of anaerobic bacteria in bacterial vaginosis is the main (but not the only) pathogenetic consequence of the complex of preceding processes. Obviously, bacterial vaginosis is a disease caused by numerous factors. Such changes in microbiocenosis occur both under the influence of exogenous and endogenous influences (Table 20-5).
Table 20-5. External and internal factors affecting changes in the vaginal microflora and contributing to the development of bacterial vaginosis
| Endogenous | exogenous |
| menopause), with the pathology of pregnancy, after childbirth, abortion (hormonal stress); - violations in the system of local immunity; - changes in vaginal antibiosis or antagonism between vaginal microorganisms; a decrease in the number of LB H2O2-producers, the concentration of hydrogen peroxide in the contents of the vagina; - hypotrophy or atrophy of the vaginal mucosa, violation of the receptors of the cells of the vaginal epithelium; - Gastrointestinal tract as a reservoir of microorganisms associated with bacterial vaginosis |
- therapy with antibiotics, cytostatics, corticosteroids, antiviral, antifungal drugs, radiation (or radiation therapy); - Violations of personal hygiene of the genital organs; - frequent and excessive vaginal showers, douching; - malformations or anatomical deformities after ruptures in childbirth, surgical interventions and/or radiotherapy; - cysts or polyps of the hymen, vaginal walls; foreign bodies in the vagina, uterus: vaginal tampons or diaphragms, pessaries, IUDs, etc.; - spermicides. |
Under the influence of endogenous and exogenous factors, the balance of the vaginal microecosystem occurs with a characteristic cascade of changes. An increased level of progesterone enhances the proliferation of cells of the vaginal epithelium, activates their receptors for bacteria. Adhesion of strict anaerobic microorganisms to the outer membrane forms "key cells". Cellular destruction along with an increase in extravasation leads to an increase in vaginal discharge.
Lower concentrations of estrogens compared to progesterone reduce the amount of glycogen in epithelial cells, as a result of which the concentration of monosaccharides and disaccharides is reduced. At the same time, the number of the pool of lactobacilli was reduced and the growth of strict anaerobes was increased. Such a mechanism is likely in some cases. Proof of this is the occurrence of bacterial vaginosis in menopause or in women after bilateral removal of the ovaries. An increase in the concentration of estrogens is also of pathogenetic significance, since it contributes to an increase in antibodies in the blood, but most importantly, it leads to hyperproliferation of the vaginal epithelium, which explains the increase in vaginal discharge.
Anaerobes produce volatile fatty acids and amino acids, which are degraded by enzymes to volatile amines. The decrease or disappearance of lactobacilli, mainly H2O2-producing, leads to a decrease in the concentration of lactic acid and an increase in the pH of the vaginal environment over 4.5. A neutral or slightly alkaline environment is more favorable for the growth of anaerobes and is not very suitable for acidophilic microorganisms. A significant place in the pathogenesis of bacterial vaginosis is occupied by the state of local immunity, which maintains the constancy of the vaginal environment. Local factors are conditionally divided into non-specific and specific. They play a leading role in protecting the genital tract from infectious diseases. Local protection of the female reproductive system is due to its anatomical and physiological features, the presence of normal microflora, the presence of lysozyme, complement, transferrin, immunoglobulins and related antibodies. Nonspecific factors of local protection of the vagina are diverse and combined into a system that includes a whole range of protection factors, such as chemical elements (zinc, copper, iron, etc.), organic substances (lysozyme, transferrin, glycoproteins, etc.), as well as a cascade the reactions they carry out.
An increase in the concentration of Na and Cl ions indicates a violation of the reabsorption function of the epithelium. It should be noted that an increase in the concentration of Na ions is also a compensatory mechanism, since a decrease in the concentration of osmotic substances (glucose and urea) is observed in bacterial vaginosis. A compensatory increase in the concentration of Na ions increases hydration, which causes profuse liquid discharge is a typical clinical sign of bacterial vaginosis. Another important factor due to an increase in the pH of the vaginal secretion is an increase in the activity of proteolytic enzymes, such as proline aminopeptidase, sialase, and mucinase, during BV. As a result, hydrolytic cleavage of protein macromolecules, including collagen, occurs, which leads to the disintegration of epithelial cells, disruption of their function and an increase in the concentration of free viable cells in the vaginal secretion.
These cells become a substrate for the vital activity of the anaerobes associated with bacterial vaginosis. Activation of the enzymes sialase and mucinase disrupts mucus formation, facilitating the accessibility of epithelial cells for microorganisms. An increase in the adhesive ability of microorganisms occurs due to the modification of cellular receptors by microbial proteases, an increase in the pH of the VJ, and a decrease in the redox potential of the vaginal epithelium. In ensuring the metabolism of anaerobes associated with bacterial vaginosis, enzymes - decarboxylases are of great importance. Their action is aimed at the decarboxylation of amino acids. The resulting carbon dioxide creates an anoxic environment. With an increase in its partial pressure, a corresponding decrease in the partial pressure of oxygen occurs. This creates the conditions necessary for the reproduction and vital activity of anaerobic microflora.
Amine test for bacterial vaginosis
One of the clinical symptoms of bacterial vaginosis is an unpleasant smell of discharge., reminiscent of the smell of "rotten fish", or a positive amine test. To conduct the test, a 10% KOH solution is added to the vaginal fluid. With a positive result, a similar unpleasant odor is determined due to the presence of volatile amines, such as: methylamine, dimethylamine, trimethylamine, cadaverine, putrescine, formed during the decarboxylation of amino acids.
The obtained data on biochemical changes in bacterial vaginosis indicate that the pathogenesis of this disease is largely determined by the imbalance between the functional activity of the vaginal epithelium, the ratio of acidophilic and other indigenous microflora and their metabolic processes. Such mechanisms are different from true inflammatory processes. This is additional confirmation of the dysbiotic nature of bacterial vaginosis.
CLINICAL PICTURE (SYMPTOMS) OF BACTERIAL VAGINOSIS
Leading and often the only symptom of bacterial vaginosis- an increased amount of whiteness, in 87% of women with an unpleasant odor, disturbing patients for a long time (on average 2 years or more).
ANAMNESIS
Examination of women begins with the collection of anamnesis. Scrupulous questioning, detailed awareness of the onset and first signs of the disease, the nature of complaints, previous treatment determine the correct diagnosis. Itching in the external genital area is noted by 26% of patients, burning - 28%, dyspareunia - 23%. Dysuric disorders are observed only in 15% of women, pain in the vagina or perineum in 21%. Regarding these complaints, 97% of women have previously repeatedly contacted a gynecologist or urologist, mycologist, endocrinologist, neuropathologist. At the same time, 95% of them were diagnosed with nonspecific vaginitis, 75% of women had previously been repeatedly and unsuccessfully treated for suspected vaginitis, while often using a variety of antibacterial drugs, both locally and orally or parenterally.
PHYSICAL EXAMINATION
During an objective examination, it is necessary to pay attention to the condition of the external genital organs, the external opening of the urethra, the mucous membrane of the vagina, the cervix, the nature of the discharge. Vaginal discharge in bacterial vaginosis, as a rule, plentiful, homogeneous, white in color, with a sharp unpleasant smell of "stale fish". Depending on the duration of the disease, the nature of the discharge is different. At the beginning of the development of the disease, leucorrhoea is of a liquid consistency, white or with a grayish tint. With prolonged bacterial vaginosis (2 years or more), the discharge is yellowish-greenish in color, thicker, resembles a curdled mass, foamy, viscous and sticky, evenly distributed along the walls of the vagina. The amount of whiteness varies from moderate to profuse, but on average their volume is about 20 ml per day (about 10 times higher than normal). A feature of bacterial vaginosis is the absence of signs of inflammation (edema, hyperemia) of the vaginal walls.
Mucous membrane with bacterial vaginosis of the usual pink color. In rare cases, in older women (in menopause), small reddish spots are found. pH measurement is carried out using indicator strips with a division scale of not more than 0.2 during the inspection. Bacterial vaginosis is characterized by a shift to the alkaline side (average 6.0). In parallel, put the reaction with a 10% solution of KOH. When mixing vaginal discharge and a few drops of alkali, the characteristic smell of “rotten fish” intensifies or appears - a positive amino test. Colposcopic picture of bacterial vaginosis characterizes the absence of diffuse or focal hyperemia, pinpoint hemorrhages, swelling and infiltration of the vaginal mucosa. In 39% of patients, pathology of the vaginal part of the cervix is found (cervicitis, ectropion, simple erosion, cicatricial deformities, etc.).
LABORATORY RESEARCH
The main laboratory research method is Gram-stained microscopy of vaginal smears from the region of the posterior fornix. Conduct microscopy of native wet smears under immersion to detect mobile microorganisms Mobiluncus spp. Microscopy evaluates various morphotypes (cocci, rods, vibrios, filamentous) of microorganisms, their gram-bearing, the presence of "key" cells, the number of leukocytes (Table 20-6) Typical symptom of bacterial vaginosis- detection in Gram-stained vaginal smears of key cells (CC). They are represented by cells of the vaginal epithelium, with gram-variable rods and cocci adhered to the membrane.
Cultural, enzyme-linked immunosorbent, serological studies, as well as DNA diagnostics, have exclusively scientific priority. Thus, it is obvious that according to a number of clinical symptoms of the disease, bacterial vaginosis can be suspected at the stage of the initial examination. Particular attention should be paid to patients who have been treated for bacterial vaginosis for a long time, but unsuccessfully, using traditional methods (soda douches, herbal medicine, antibiotic therapy, etc.). Persistent leucorrhea against the background of long-term antibacterial and anti-inflammatory therapy is an important diagnostic criterion for bacterial vaginosis.
DIFFERENTIAL DIAGNOSIS OF BACTERIAL VAGINOSIS
Differential diagnosis of bacterial vaginosis is presented in Table. 20-6.
The principal goal of therapy is to resolve vaginal symptoms. All women with symptoms of bacterial vaginosis need treatment. The use of metronidazole in bacterial vaginosis significantly reduces the incidence of PID after abortion. Therefore, treatment of bacterial vaginosis (symptomatic or asymptomatic bacterial vaginosis) is necessary before performing surgical abortions.
MEDICAL TREATMENT OF BACTERIAL VAGINOSIS
To date, a two-stage method for the treatment of bacterial vaginosis is generally recognized. Its principle is the creation of optimal physiological conditions for the vaginal environment and the restoration of microbiocenosis. At the first stage of treatment, local antibacterial therapy is carried out (clindamycin vaginal cream 2%, metronidazole, chlorhexidine, etc.), lactic acid is prescribed to lower the pH, immunocorrectors (if indicated), estrogens, prostaglandin inhibitors and antihistamines. In the presence of itching, burning, pain, local anesthetics are used.
- Treatment regimens recommended by the US STS Control Board(1998) and adapted to the conditions of our country for the treatment of non-pregnant women (stage 1):
Chlorhexidine (hexicon ©) 1 vaginal suppository 1-2 times a day for 7-10 days
- clindamycin - vaginal cream 2% one full applicator (5 g) intravaginally at night for 7 days;
- or clindamycin - vaginal suppositories, 1 vaginal suppository 1 time per day for 3-6 days;
- or metronidazolegel 0.75% one full applicator (5 g) intravaginally - 1-2 times a day for 5 days;
- or metronidazole 500 mg orally 2 times a day for 7 days;
-or tinidazole 500 mg orally 2 times a day for 5 days;
-or ornidazole 500 mg orally 2 times a day for 5 days.
Patients should be warned that they should avoid drinking alcohol during treatment with metronidazole and its analogues, as well as within 24 hours after the end of treatment. Clindamycincrem is oil based and can damage the structure of latex condoms and diaphragms.
In 2006, at the RSMC. N.I. Pirogov under the guidance of Professor E.F. Kira conducted an open randomized comparative study of the efficacy and safety of Hexicon © (chlorhexidine bigluconate 16 mg), vaginal suppositories and Flagyl © (metronidazole 500 mg), vaginal suppositories in the treatment of bacterial vaginosis.
A primary evaluation of the effectiveness (on the 8th and 12th day after completion of treatment) and a secondary evaluation were carried out. Particular attention was paid to the effect of Hexicon© and Flagyl© on lactobacilli. The drugs were prescribed according to the schemes: Hexicon© 1 suppository 2 times a day for 7–10 days and Flagyl© 1 suppository 2 times a day for 10 days. The effectiveness of Hexicon © in the treatment of bacterial vaginosis was 97% of patients immediately after treatment with Hexicon ©, Flagyl © - 83%. A month after treatment, clinical and laboratory recovery occurred in 97% of patients treated with Hexicon, and in 93% of patients using Flagyl©. Unlike Flagyl ©, Hexicon © helps to improve the species composition and quantity of lactic acid bacteria. Inoculation of lactobacilli in the treatment with Hexicon © increased from 31% to 51%, for bifidobacteria from 10% to 19%.
Hexicon© was well tolerated by the patients, no adverse events were registered.
- Alternative regimens for bacterial vaginosis (first stage): -metronidazole 2 g orally once or -tinidazole 2 g orally once or -ornidazole 2 g orally once or - clindamycin 300 mg orally 2 times a day for 7 days.
Relapses of bacterial vaginosis are quite common. Alternative regimens are used to treat relapses of BV. There is currently no regimen for the treatment of bacterial vaginosis using any drug for long-term maintenance therapy. Clinical trials have shown that treatment of sexual partners does not affect either the success of treatment in a woman or the frequency of relapses, therefore routine treatment of sexual partners is not recommended.
If you are allergic to metronidazole (and analogues) or intolerant to it, clindamycin cream can be used for treatment. Metronidazole gel is prescribed for patients with intolerance to systemic metronidazole, however, patients with an allergy to oral metronidazole should not be given intravaginally.
The second stage of treatment of bacterial vaginosis involves the use of bacterial biological preparations: lactobacillus acidophilus, acylacta, bifidobacteria bifidum, bifidine, etc. locally or lactogen inside to restore the vaginal microflora. The appointment of these drugs without a preliminary first stage is futile due to the pronounced competition between vaginal microorganisms. When carrying out complex etiotropic and pathogenetic therapy of bacterial vaginosis, a positive result is achieved in 90%. There are currently no standards for the restoration of the vaginal biocenosis. Below in table. 20-7 shows the main eubiotics and probiotics used to correct the vaginal microflora.
Table 20-7. Eubiotics and probiotics used to correct the vaginal biocenosis
* Not produced commercially. Has historical significance.
** Capsules for oral use.
Bacterial vaginosis therapy with eubiotics usually begins 2-3 days after the end of the first (antibacterial) treatment. During this time, elimination from the vagina or the body of antibacterial agents introduced at the first stage occurs. This excludes the so-called "post-antibiotic effect", that is, a decrease in the effectiveness of eubiotics due to exposure to trace concentrations of antibacterial drugs.
INFORMATION FOR THE PATIENT
The patient is informed about the adverse effects of bacterial vaginosis. Regular gynecological examinations are recommended.
FORECAST
With timely diagnosis and adequate treatment of bacterial vaginosis, the prognosis is usually favorable.
Today we will talk about:
Vaginosis- This is a pathological condition of the vaginal mucosa of non-inflammatory origin, caused by the replacement of normal microflora with anaerobic microorganisms. There is no specific causative agent for vaginosis. Among the causes that provoke it, there are many different microorganisms, but their presence does not provoke local inflammatory changes in the vagina. It is on this feature of the course of the disease that the differential diagnosis of vaginosis is based.
The causes of vaginosis are not well understood, and the question of whether it belongs to diseases continues to be discussed. The only condition for the development of vaginosis is a change in the parameters of normal vaginal microbiocenosis and, as a result, a violation of the mechanism for protecting mucous membranes from unwanted microorganisms.
To understand the essence of the pathological processes in vaginosis, it is necessary to have a clear idea of how the vaginal epithelium functions, and by what mechanisms it protects the reproductive system from potential infection.
The vagina connects the uterus (and indirectly, the appendages) with the external environment and therefore is in a state of constant resistance to its negative influence in order to protect the internal genitalia from inflammation.
The vaginal wall is formed by three layers: connective tissue, muscle and epithelial. The vaginal epithelium is formed by layers of squamous cells, its uppermost layer (the one that lines the inside of the uterine cavity) is in a state of constant renewal. Every month, according to cyclical changes in other genital organs, the surface layer of the vaginal epithelium is shed (sloughed off) and replaced by new cells. Thus, the mucosa is "cleared" of the potential cause of inflammation and protects the upstream organs from infection.
The key to successful mucosal barrier function is the constancy of the vaginal microenvironment. In a healthy vagina, it is represented by a dominant amount (98%) of lactobacilli and a small population of opportunistic microorganisms. The quantitative superiority of lactoflora provides reliable protection of mucous membranes from infection. If there are fewer lactobacilli, opportunistic microbes take their place.
In order to provide themselves with a numerical advantage, lactobacteria create conditions unsuitable for the vegetation of "harmful" microorganisms. They attach to the membranes of desquamated cells of the surface epithelium and “extract” glycogen from them, and then synthesize lactic acid from the latter. As a result, a constant level of acidity is maintained in the vagina (3.8 - 3.5). In an acidic environment, opportunistic flora is not able to compete with lactobacteria, therefore it remains small and safe.
Vaginosis is formed in the event that, against the background of a quantitative decrease in lactobacilli and a change in acidity (pH), populations of opportunistic microorganisms begin to multiply in the vagina, i.e. in fact, it is a local dysbiotic disorder.
Thus, vaginosis is formed due to "its own" microflora, which is constantly present in the vagina of any healthy woman. It is impossible for them to "get infected" or betray a partner during intimacy.
Acute vaginosis is rarely diagnosed. Since vaginosis does not provoke pronounced inflammation, the disease often does not have active subjective complaints. The pathological process in the mucous membranes of the vagina is able to proceed erased, then aggravating, then fading again.
Chronic vaginosis depletes local immunity and can cause inflammation when, against the background of a significant decrease (or complete disappearance) of lactoflora, unwanted microorganism begin to multiply excessively in the vagina.
Perhaps the only symptom of vaginosis is abnormal discharge. Their color and consistency depend on which microflora displaces lactobacilli, how long vaginosis exists, and what background processes occur in the surrounding tissues.
Diagnosis of vaginosis is based on visual examination of the mucous membranes and laboratory examination of the vaginal discharge. By studying the microbial composition of vaginal leucorrhoea, the severity of the disease is determined: the less lactobacilli in the material, the more severe the vaginosis.
Therapy of vaginosis does not have a clearly defined plan. Each regimen for the treatment of vaginosis is the result of an individual study of the clinical situation. As a rule, treatment is aimed at eliminating unwanted microbial flora and restoring the lactobacillus population. Inside pills for vaginosis are prescribed according to indications. Preference is given to a local preparation (ointments, creams, suppositories).
Vaginosis often recurs. Prevention of vaginosis and its recurrence consists in the exclusion of provoking factors and a reasonable attitude towards sexual life.
The cause of the formation of vaginosis is its own opportunistic microflora present in the vagina of a healthy woman. Perhaps this is the uniqueness of vaginosis: the body independently provokes the disease without the involvement of external resources.
The microbial composition of the vaginal environment for each individual woman is individual, so it is impossible to name the only culprit in the development of vaginosis. It is provoked by polymicrobial complexes, which consist mainly of anaerobic microorganisms (mainly coccal nature). More often, with vaginosis, corynebacteria, mycoplasmas, epidermal staphylococcus aureus, lactic acid streptococci and other microbes prevail in the vaginal contents. It should be noted that the previously existing idea of the dominant role of gardnerella in the pathogenesis of vaginosis has now been refuted by numerous studies. It turned out that gardnerella colonize the vagina in more than 50% of healthy women, without causing pathological dysbiotic changes in the habitat. Obviously, this microorganism acts as a pathological agent only if it is associated with another microflora.
Factors provoking dysbiotic disorders in the vagina are:
Incorrect hygiene measures. Some patients use douching too often, during which the “useful” microflora is simply mechanically washed off the surface of the mucous membranes. Also, aggressive cosmetics (soaps, gels) that are not suitable for intimate care have a negative effect on the vaginal epithelium.
The lack of proper intimate hygiene can also provoke vaginosis, as many unwanted microbes and their waste products accumulate on the mucous membranes.
Irrational antibiotic therapy. Free access to the purchase of antibiotics (including very "strong" ones) has very negative consequences: without the participation of a qualified medical examination, the sick are treated on their own, not always choosing and taking medicines correctly.
Antibiotic therapy prescribed by specialists always involves measures to prevent dysbiotic disorders and rarely leads to the formation of vaginosis.
Hormonal dysfunction. All ongoing processes in the vaginal mucosa are closely related to cyclic hormonal fluctuations. The state of the vaginal microflora is affected by the level of estrogens, they support the processes of renewal of the surface mucous layer, providing lactobacilli with a sufficient amount of glycogen. Under conditions of hypoestrogenism (especially long-term), the mucous layer becomes thinner, the population of lactobacilli decreases, and conditionally pathogenic microorganisms begin to vegetate intensively.
Changes in the normal hormonal background are more likely to explain vaginosis in pregnant women, women in menopause, or in women who have had a recent abortion.
Taking hormone-containing medications or contraceptives can also contribute to the appearance of vaginosis.
- Unprotected intimate relationships with different partners. In addition to an increased likelihood of getting a venereal infection, promiscuity leads to serious changes in the composition of the vaginal microflora and depletes local immunity. Moreover, the number of sexual partners increases the risk of vaginosis much more than the number of unprotected sex.
- Intestinal dysbacteriosis. Symmetric dysbiosis of the intestinal and vaginal mucosa is often diagnosed, especially against the background of endocrine diseases or antibiotic therapy. Every second patient with vaginosis has a diagnosed intestinal dysbacteriosis.
- Violations of immunological reactivity. The cause of vaginosis can be systemic allergic diseases or short-term local allergic reactions, for example, to hygiene products (vaginal tampons, soap, etc.), intimate lubricant, latex or talc contained in condoms.
- Intrauterine contraception (spiral). It provokes the appearance of vaginosis quite often (52%). Obviously, the spiral is perceived by the mucous membranes as a foreign body, and they respond to its presence with a local allergic reaction. In addition, any (even the most “good”) intrauterine contraception serves as a source of local non-infectious inflammation. In order for the intrauterine contraceptive to fulfill its intended purpose without accompanying negative manifestations, it is necessary to follow simple medical recommendations and not leave it in the uterine cavity for longer than the prescribed period.
Whatever the causes of vaginosis, a short-term change in the normal composition of the vaginal microflora in most healthy patients is eliminated through self-regulatory mechanisms. The disease develops only if the body is unable to eliminate local dysbiosis on its own.
Symptoms and signs of vaginosis
Vaginosis is distinguished by poor symptoms and the absence of specific clinical signs. Often the disease proceeds without pronounced subjective signs and does not prompt the patient to consult a doctor.
The leading, and sometimes the only, symptom of vaginosis is pathological discharge (leucorrhoea). Their number and appearance depend on several factors, one of which is the duration of the disease.
Acute vaginosis is accompanied by abundant white liquid leucorrhoea, sometimes the vaginal discharge has a grayish tint and an unpleasant odor. More often, an acute process occurs after hypothermia, severe emotional shock, allergic reactions, due to antibiotic therapy.
Chronic vaginosis can exist for years. If dysbiotic disorders in the vagina last more than two years, the discharge becomes thick and sticky, and its color changes to yellow-green. The change in the nature of leucorrhea in chronic vaginosis is associated with the degree of local dysbiosis: the longer vaginosis lasts, the less lactobacilli remain in the vagina, and the more pronounced the influence of opportunistic microflora. Long-term vaginosis significantly depletes the mechanism of local protection of the mucous membranes and can often cause the attachment of secondary pathological microflora and the development of infectious inflammation.
Allocations with vaginosis have one specific difference - an unpleasant odor, reminiscent of the smell of stale fish. It is “provided” by anaerobic bacteria competing with lactoflora. They synthesize substances (amines), which decompose with the release of an unpleasant, "rotten" odor. Often the patient is brought to the doctor not by the presence of whites, but by their unusual smell.
The clinic of vaginosis also depends on the state of hormonal function, in particular, on the level of estrogen. Lower (in comparison with progesterone) concentrations of estrogens lead to a decrease in glycogen content in the vaginal epithelium. Since less lactobacilli are required to process a small amount of glycogen, their number decreases, and anaerobic microflora occupies the vacated place on a competitive basis. Prolonged lack of proper estrogenic influence provokes thinning of the mucous layer of the vagina (orthia). The vagina becomes "dry", easily vulnerable, so the amount of whiteness against the background of vaginosis decreases, and the patient has subjective complaints of discomfort, dryness, burning and / or itching. Similar ones are typical for women with physiological (older age) or artificial (removal of the ovaries) menopause.
Diagnosis of vaginosis does not require a large number of examinations, however, the analysis of the data obtained is associated with some difficulties. Vaginosis should be distinguished from vaginitis, which, unlike the latter, is the result of an infectious inflammation of the vaginal mucosa. Often, patients treat non-existent vaginitis for years, using antibiotics, which only aggravate vaginal dysbiosis and lead to the development of chronic vaginosis.
The diagnosis of vaginosis is confirmed by several reliable criteria:
- Absence of inflammatory changes in the vaginal mucosa. On visual examination, the mucosa has the usual "healthy" appearance and pink color. In the vagina there is an increased amount of light discharge without external signs of the presence of pus, often (87%) during examination, their unpleasant odor is felt.
- Change in the acidity of the vaginal environment. To measure pH quantitatively, special indicator test strips are used. The division scale applied to them with vaginosis indicates a characteristic shift in acidity to the alkaline side (more than 4.5).
Changes in the microbial composition of the vaginal discharge according to the results of laboratory diagnostics. In smears, there is no increased number of leukocytes inherent in inflammatory diseases, but there is a quantitative shift in the microbial composition: against the background of a decrease (or complete absence) of lactoflora, an excessive increase in populations of opportunistic microorganisms is observed.
Among other anaerobic bacteria, a large number of Gardnerella are often found. In acceptable quantities, their population is completely harmless to the mucous membranes, but under conditions of pronounced dysbiosis, gardnerella enter into microbial associations and “help” maintain the pathological process. The simple detection of Gardnerell in a smear does not have independent significance.
The presence in the smear of the so-called "key cells". Microscopy of the vaginal discharge with vaginosis often visualizes a large number of desquamated epithelial cells with microbes adhering to their membranes. They are called "key".
Thus, the diagnosis of vaginosis is confirmed by:
- specific vaginal discharge (often with a "fishy" smell);
- increased above 4.5 vaginal pH;
- positive "amine test";
- key cells in the smear.
In 40% of patients with signs of vaginosis, when viewed on the cervix, background diseases (cervicitis, ectropion, scars) are found, more often pseudo-erosion. They often change the clinic of vaginosis and require additional colposcopic examination.
Despite the meager symptoms, the presence of vaginosis can be suspected at the stage of studying the clinical symptoms. Often in a conversation, patients point to a long, unsuccessful treatment of the so-called "inflammation" of the vagina. They may also note that the next course of anti-inflammatory therapy does not eliminate, but exacerbates negative symptoms.
In recent years, patients often face the conclusion of "cytological vaginosis". Unlike the usual, cytological vaginosis is the result of excessive reproduction of lactobacilli. This condition is often provoked by intimate hygiene products with an acidic pH, especially if they contain lactobacilli. Sometimes this type of vaginosis can appear against the background of hyperestrogenism. Excess estrogen stimulates excessive production of glycogen, which requires more lactobacilli to utilize.
Clinically, cytological vaginosis resembles candidal vaginitis, when, against the background of vaginal discomfort, burning or itching, abundant white "curdled" discharge appears. Both conditions are clinically so similar that diagnostic errors often occur.
It is possible to differentiate cytological vaginosis from according to the following criteria:
- vaginal pH less than 3.5;
- microscopically: many cells of the destroyed epithelium in the form of fragments against the background of a large number of lactobacilli;
- false key cells: instead of opportunistic microbes, lactobacilli are attached to the surface of epithelial cells, imitating true key cells;
- cultures and smears for the presence of candidal fungi are negative;
- no signs of inflammation (white blood cells are normal) in smears.
Vaginosis during pregnancy
Pregnancy is sometimes (20 - 46%) one of the physiological causes of vaginosis, as it creates favorable conditions for the formation of local dysbiotic disorders: a decrease in the amount of estrogens and a significant depletion of immune defense mechanisms.
In half of the cases, the disease does not cause pathological subjective sensations, and an increased amount of vaginal discharge is accepted by the pregnant woman as the norm.
The only reliable symptom of vaginosis in pregnant women is abundant liquid leucorrhoea with an unpleasant odor. If the discharge continues for a long time, the patient may notice a change in their consistency from liquid to thick, and in color from white to yellowish. Often in a conversation it turns out that episodes of the appearance of such whites were observed even before pregnancy.
Diagnosis of vaginosis in pregnant women is similar to that in non-pregnant women and includes examination of complaints (if any), visual examination of the vaginal mucosa, and laboratory examination of vaginal contents. An amine test and a vaginal pH measurement are also performed.
Pregnant women are examined for the presence of vaginosis three times: at the first visit, before maternity leave (27-30 weeks) and on the eve of childbirth. In the case of a positive result after the course of therapy, an additional examination is carried out to monitor the cure.
Vaginosis during pregnancy can provoke an infectious inflammation. Against the background of reduced immunity, an infection from the vagina can rise into the cervical cavity and uterus. And although the likelihood of such a scenario is small, it is impossible to leave vaginosis in pregnant women unattended.
The treatment regimen for vaginosis in pregnant women is characterized by the predominant use of local therapy. Systemic drugs are used infrequently and only in the second half of pregnancy.
Treatment of vaginosis
Unfortunately, many women leave the signs of vaginosis unattended or try to get rid of it on their own. Self-treatment on the principle of therapy for inflammatory diseases of the vagina not only does not help, but also aggravates the course of vaginosis. Randomly selected antibacterial agents only exacerbate the course of vaginosis, and "useful" douching literally wash out the remnants of microflora from the surface of the vagina.
To cure vaginosis, it is necessary to consistently eliminate its causes: remove the unfavorable background that provokes dysbiosis in the vagina; destroy the excessively multiplied opportunistic microflora and restore the normal amount of lactobacilli.
To choose the right treatment tactics, it is necessary to take into account the severity of vaginosis. It is measured by the amount of lactoflora remaining in the vagina and the microbial composition of the vaginal environment.
Conventionally, there are three significant degrees of severity of vaginosis:
- The first degree of severity (compensated vaginosis) is characterized by the complete absence of microflora in the test material, the presence of unchanged, normal, vaginal epithelium. The cause of such vaginosis may be excessive intimate hygiene or antibiotic therapy. Compensated vaginosis does not always require detailed therapy, sometimes the body independently copes with a temporary violation of the microbial balance after the disappearance of the cause of its appearance.
- The second degree (subcompensated) severity of vaginosis is characterized by a decrease in the number of lactobacilli, a quantitative increase in the population of anaerobic bacteria and the manifestation of key cells in a small amount (up to five in the field of view).
- Decompensated (third) degree of severity is manifested by a pronounced clinic of vaginosis, the complete absence of lactobacilli against the background of a large number of microbial populations and a significant number of key cells (covering the entire field of view).
After the unwanted infection is eliminated, a niche is released in the vaginal environment, which must be occupied by lactobacilli. At the second stage of treatment, favorable conditions are created for restoring normal microbial balance with the help of eu- and probiotics, which contain lacto- and bifidobacteria.
Two-stage treatment of vaginosis is successful in 90% of cases, but it does not guarantee the absence of recurrence of the disease. Relapses of vaginosis are treated similarly to the acute process. To avoid the return of vaginosis, simple preventive measures should be observed. Prevention of vaginosis involves:
- adequate intimate hygiene;
- rational antibiotic and hormone therapy;
- prevention (or treatment) of intestinal dysbiosis;
- culture of sexual life: restriction of sexual partners and use of barrier contraception;
- regular examinations in the conditions of the antenatal clinic.
- Candles and preparations for vaginosis
The choice of medicine depends on which microorganisms are found in the material during laboratory testing.
The local method of administering the drug is preferable, therefore, the following are more often prescribed: Chlorhexidine in solution or Hexicon vaginal suppositories; suppositories or cream Clindamycin (Metronidazole), Flagyl suppositories.
An alternative to local treatment is taking Metronidazole, Tinidazole, Ornidazole tablets according to the scheme chosen by the doctor.
Bacterial vaginosis is a condition in which there is a violation of the quantitative and qualitative composition of the microflora of the vagina. According to various data, about 20 percent of women of reproductive age suffer from this disease. This disease may not manifest itself for a long time. In some cases, external manifestations in the form of secretions from the genital tract with a pungent odor can be so pronounced that it makes a woman seek help from a gynecologist at the very debut of the disease. Unfortunately, timely seeking medical help is not always the key to successful treatment. The reason for the failure in the treatment of this disease is the many factors that can cause vaginosis.
What is the normal microflora of the vagina?
In the lumen of the vagina, the processes of growth and development of various types of bacteria and fungi are constantly taking place. Their vital activity should normally be constantly monitored by the body of the woman herself with the help of changes in the hormonal background, immune changes and under the influence of the intestinal microflora. In some cases, a violation in the process of monitoring the composition of the microflora leads to a persistent change in the properties of the vaginal mucus, and can lead to damage to the mucous epithelium itself.Normally, the vast majority of vaginal bacteria are lactobacilli, which are also called Doderlein sticks. These bacteria are represented by 4 species: Lactobacillus acidofilus, Lactobacillus Casei, Lactobacillus Fermentum, Lactobacillus cellobiosus. These bacteria have a number of properties inherent only to them: they produce peroxides that form an acidic environment in the vagina (normal pH is 3.8-4.4) and prevent the reproduction of other types of microorganisms in the vaginal lumen.
How does the body control the microflora of the vagina?
Hormonal systemThe number and composition of the microflora is controlled by the hormonal background: when it changes, the number of receptors on the surface of epithelial cells, to which bacteria can attach, changes. Also, the rate of renewal of the epithelium of the vaginal mucosa is controlled mainly by the hormonal background.
The immune system
It controls the microflora due to the secretion of IgA antibodies. On the surface of the cells of the vaginal mucosa, this immunoglobulin prevents bacteria from attaching to epithelial cells, which prevents the penetration of bacteria into the cell or into the layers of the mucous epithelium. With infectious inflammation, the army of leukocytes immediately moves into the lumen of the vagina to destroy the pathogenic or conditionally pathogenic microflora that caused the inflammation.
Properties of lactobacilli
Naturally, most of the bacteria colonizing the vaginal mucosa tend to create an environment that would be most favorable for their own development and unsuitable for the reproduction and development of competitors. Due to the ability of lactobacilli to secrete hydrogen peroxide, a rather acidic environment is created, which is unsuitable for life for many pathogenic bacteria.
What is vaginosis?
Vaginosis is a violation of the composition of the microflora of the vaginal mucosa that does not cause an inflammatory reaction. The clinical symptoms of such a disorder can be different - from the complete absence of symptoms, to pronounced discharge with an unpleasant odor, with a feeling of itching and discomfort.
Causes of bacterial vaginosis
- Violation of the hormonal background. A number of gynecological and endocrinological diseases are accompanied by a violation of the cyclical change in the concentrations of female sex hormones in the blood. Violation of the hormonal background leads to changes in the renewal of the vaginal epithelium, the properties of the cells of the vaginal epithelium.
- Decreased immunity. Violation of the activity of the immune system leads to a decrease in the ability of the immune system to influence the composition of the microflora, the activity of the synthesis of secretory antibodies, the activity of immune cells decreases.
- Violation of the intestinal microflora. A change in the bacterial composition of the intestine leads to a change in the composition of the microflora of the vagina. Therefore, intestinal dysbacteriosis can serve as the main cause of vaginosis.
- Use of antibiotics- in some cases, it can lead to a change in the qualitative and quantitative composition of the vaginal mucus. The thing is that antibiotics do not have a selective effect on certain types of bacteria. For example, in the treatment of bronchitis, along with the destruction of the bacteria of the bronchial tree, the antibacterial drug also destroys the beneficial microflora of the intestines and genital tract.
Symptoms of bacterial vaginosis
The severity and list of symptoms can vary widely depending on the composition of the microflora and the state of the body.- Abundant or scanty discharge from the genital tract. More often, the discharge is purulent, white in color, with an unpleasant pungent odor, the discharge is more active after sexual contact or during menstruation.
- Itching is constant, may intensify during menstruation.
- Pain during genital intercourse. This symptom can be caused by a change in the mucous epithelium of the vagina and the aggressive properties of the vaginal microflora.
- Adhesion of the labia minora - associated with the active release of pus.
- Burning sensation during urination - this symptom rarely occurs and may be associated with irritation of the mucous membrane of the external urethra.
Diagnosis of bacterial vaginosis
 Diagnosis of bacterial vaginosis is based on the symptoms of the disease, signs detected during a gynecological examination and laboratory analysis data.
Diagnosis of bacterial vaginosis is based on the symptoms of the disease, signs detected during a gynecological examination and laboratory analysis data. The symptoms of bacterial vaginosis are listed in the previous chapter of the article.
Gynecological examination
On examination, the gynecologist reveals abundant purulent discharge of their genital tract, in some cases the labia are glued together with drying pus. When viewed in the mirrors, pus can be detected on the surface of the mucosa.
Laboratory research
Microscopic examination of a smear from the vaginal mucosa- is the main method in the diagnosis of vaginosis. A smear is taken from the posterior surface of the vaginal part of the cervix during a gynecological examination in the mirrors. After staining with special reagents, the smear is examined under a microscope. Most of the known bacteria that actively colonize the uterine mucosa in vaginosis can be identified as a result of this examination. The sensitivity of this method reaches 100%.
Bacteriological research not as effective in diagnosing the cause of vaginosis. However, this method in some cases is indispensable for diagnosing concomitant infectious lesions.
Amino test effective for express diagnosis of vaginosis caused by anaerobic bacteria. As a result of the vital activity of these bacteria, organic substances such as putrescine, cadaverine, trimethylamine are released into the external environment. These substances create the smell of "spoiled fish".
DefinitionspH vaginal secretion. Revealing a pH over 4.5 is one of the signs of vaginosis. As we said above, low pH values in an acidic environment provide beneficial bacteria (Doderlein sticks). A decrease in acidity indicates that their number is reduced.
Treatment of bacterial vaginosis
 Bacterial vaginosis is treated in stages. At the first stage, the causes that caused the violation of microflora are eliminated: hormonal correction, stimulation of immunity, normalization of digestion, elimination of anatomical defects of the external genital organs.
Bacterial vaginosis is treated in stages. At the first stage, the causes that caused the violation of microflora are eliminated: hormonal correction, stimulation of immunity, normalization of digestion, elimination of anatomical defects of the external genital organs. The second and third stages are standard for all types of vaginosis:
Use of antibiotics
Restoration of the numerical and qualitative composition of the normal microflora of the vagina

Restoration of normal microflora is a complex process. Basically, preparations containing live cultures of lactobacilli are used for this purpose.
It is important to note that the use of local forms of eubiotics (in the form of vaginal suppositories) does not always bring the expected result. Therefore, the recommendations are reduced to an integrated approach - the intake of eubiotic preparations orally and the local use of drugs in this group.
The duration of treatment is determined by the attending gynecologist individually, depending on the results of the intermediate diagnosis and the dynamics of the process.
The effectiveness of the treatment can be assessed only 4-6 weeks after the end of the course of treatment. The main criterion for the normalization of microflora is a quantitative and qualitative bacteriological examination of a smear from the vaginal mucosa.
Prevention of bacterial vaginosis
The most important thing in preventing the recurrence of bacterial vaginosis is the exclusion of predisposing factors:- Rational use of antibiotics.
- Maintaining the intestinal microflora at a normal level (prevention of intestinal dysbacteriosis).
- Normalization of the hormonal background (treatment of hormonal gynecological diseases).
- Maintaining the protective properties of the body (immunity) at a high level
- In some cases, the use of vaginal hygiene products and contraceptives should be excluded.

How to treat vaginosis during pregnancy?
 According to statistics, every fifth pregnant woman develops vaginosis. Such a frequent occurrence of this pathology is explained by the following facts: during pregnancy, the number of "useful" lactic acid bacteria in the woman's vagina is significantly reduced. In addition, the body's defenses are weakened. As a result, the microflora can no longer withstand the onslaught of pathogenic microbes, and vaginosis develops.
According to statistics, every fifth pregnant woman develops vaginosis. Such a frequent occurrence of this pathology is explained by the following facts: during pregnancy, the number of "useful" lactic acid bacteria in the woman's vagina is significantly reduced. In addition, the body's defenses are weakened. As a result, the microflora can no longer withstand the onslaught of pathogenic microbes, and vaginosis develops. For the treatment of vaginosis during pregnancy, drugs containing metronidazole. In this case, vaginal remedies are preferable to tablets that must be taken orally. It is especially convenient to use the gel with metronidazole (it is inserted into the vagina with a special syringe). The drug is used once a day at bedtime for 7 days.
Equally effective and convenient is metronidazole in the form of vaginal pills ( Klion-D) to be inserted deep into the vagina at bedtime for 10 days.
For the treatment of vaginosis in pregnant women, drugs such as Trichopolum, Metrogil, Tiberal, Ornitazol produced in various forms.
All of these drugs are used only after 20-22 weeks of pregnancy, when they cannot harm the developing fetus.
In the earlier stages of pregnancy, treatment of vaginosis with antimicrobial drugs is prescribed only in case of a real threat to the health of the mother and fetus.
In addition to specific drugs, in the treatment of vaginosis, pregnant women must be prescribed drugs containing lactobacilli. They are used both inside and in the form of douching. They are useful not only for restoring the microflora of the vagina, but also for the female body as a whole.
Treatment of vaginosis in a pregnant woman can only be carried out as directed and under the supervision of a gynecologist.
What suppositories are effective in the treatment of vaginosis?
| Name of the drug | Mechanism of action | Dosage and mode of application |
| neo-penotran(Neo-penotran forte) | The composition of the drug includes metronidazole and miconazole. Because of this, it has antibacterial and antifungal properties. It can be used even during pregnancy, in the second half. | It is introduced into the vagina one vaginal suppository at night for 10 days. |
| Hexicon(Chlorhexidine, Hexicon D, Katejel, Tsiteal, Plivasept) | Preparation containing chlorhexidine. It has antibacterial activity, but it does not interfere with the activity of lactic acid bacteria. | It is used for 10 days, 1-2 suppositories in the vagina (depending on the severity of the current). |
| Metronidazole(Metrogil, Flagyl, Trichopolum, Efloran) | Antibacterial drug, effective in almost all types of vaginosis, including those caused by Trichomonas. | Dosage - 1 suppository in the vagina at night, for 5-7 days. |
| Clindamycin(Klindacin, Zerkalin, Clindafen, Dalacin, Klimitsin) | A drug based on the antibiotic clindamycin. Effective in bacterial vaginosis. | Assigned to one vaginal suppository 1-2 times a day. In severe cases, the dose may be increased. The duration of the course is 7-10 days. |
| Bifidumbacterin | Contains live bifidobacteria; restores the normal microflora of the vagina. | Introduced into the vagina 1 suppository at night. The course of treatment is 10 days. |
| Ecofemin | A preparation containing live lactobacilli to restore normal microflora. | Suppositories are inserted into the vagina 2-3 times a day. The course of treatment is 10 days. |
How to treat vaginosis at home?
 There are a large number of ways to treat vaginosis at home.
There are a large number of ways to treat vaginosis at home. - In the initial stages, douching can be dispensed with. For this, a 2-3% solution of lactic or boric acid is suitable. For the procedure, it is enough to take a large syringe. The solution should be warm, but not hot. Procedures can be carried out 1-2 times a day. Efficacy depends on how early treatment is started. If the symptoms of vaginosis are not particularly pronounced, then douching will be enough, but in any case, tests should be taken after treatment.
- Medicines can be injected into the vagina using tampons. To do this, a cotton swab is moistened with the selected agent (it can be a solution of ascorbic or lactic acid; ointment with metronidazole or tinidazole; lactobacterin) and inserted deep into the vagina. The duration of the procedure is 15-20 minutes. After that, remove the swab and do not wash. The effect appears after 3-4 procedures. To achieve the desired result, you need to do 10 procedures.
- It is especially convenient to use vaginal tablets or suppositories. It can be Klion-D, Metronidazole, Vaginorm, Ecofemin, Klevazol, etc. A tablet or suppository should be inserted deep into the vagina. The duration of treatment depends on the type of drug and is indicated in the instructions. Signs that the remedy really helps will appear in a couple of days. As a rule, the itching decreases, and the discharge disappears. But do not give up treatment; you need to complete a full course of 7-10 days.
What are the traditional methods of treating vaginosis?
 You can cope with vaginosis with the help of folk methods. Of course, the treatment in this case will be longer, but there are no side effects. Signs of improvement when using folk remedies appear after 2-2.5 weeks of regular use.
You can cope with vaginosis with the help of folk methods. Of course, the treatment in this case will be longer, but there are no side effects. Signs of improvement when using folk remedies appear after 2-2.5 weeks of regular use. Infusions of medicinal plants for oral use:
- Mix equal amounts of leuzea and marshmallow roots, as well as pine buds, sweet clover grass, wormwood, cudweed, lavender. Two tablespoons of the mixture is poured with a liter of boiling water. After 6 hours, you can take the infusion inside half a glass before meals three times a day. The treatment lasts three months.
- Also inside you can use an infusion from the following mixture: elecampane roots, birch leaves, mint, chamomile, licorice, thyme, geranium and meadowsweet in equal amounts. The method of preparation and dosage are similar to those described above.
- You can try the following mixture: lingonberry leaves, knotweed, elecampane, viburnum, lavender, plantain, tansy, leuzea and mistletoe, taken in equal parts. The solution is prepared in the same way as in the previous recipes.
- Another option is to mix equal amounts of dry herbs of bergenia, knotweed, calendula, angelica, nettle, toadflax, coltsfoot; chicory and dandelion roots. Apply as in previous recipes.
- Mix dry crushed blueberry, cuff, birch, tansy and Greek leaves taken in equal amounts. Two tablespoons of the mixture is brewed with one liter of boiling water and infused for 6-8 hours. After this, the infusion must be filtered and used for douching or vaginal tampons, wetting the tampon with infusion and inserting it deep into the vagina. The procedure is carried out daily up to 2-3 times a day. One procedure will require a glass of infusion.
- Mix in equal proportions oak bark, geranium herbs, wormwood, chamomile and violets. The infusion is prepared in the same way as in the previous recipe. It is used in the form of douching or tampons.
- A mixture of the roots of mountaineer serpentine, Veronica grass, plantain, yarrow, thyme, calendula flowers and bird cherry leaves. The components are mixed in equal amounts. The infusion is prepared in the manner described above. Used for douching.
- Marshmallow roots, St. John's wort, marigold flowers, meadowsweet grass, dandelion leaves and blueberries are mixed in equal amounts. The infusion is prepared by the method described above. It is used in the form of douching or tampons.