Treatment after shoulder dislocation. Rehabilitation and treatment of shoulder dislocation after reduction. Mechanism of injury
Contents of the article: classList.toggle()">toggle
A shoulder dislocation is a fairly serious injury in which the surfaces of the bones in that area partially or completely stop touching each other.
It is almost impossible to correct the situation on your own; this requires the help of a doctor. In some cases, after the dislocation is reduced, problems with the shoulder joint remain.
Shoulder Dislocation and the Army
In 80% of young patients, shoulder dislocation occurs again. This situation can be corrected through surgery. Young men who are required to serve in the army should consult a doctor after each case of dislocation to obtain supporting medical documents.
If a patient has joint dislocations more than 3 times a year, he has all the supporting documents and x-rays of the joint before and after reduction of the dislocation, then he can be assigned category B (limitedly fit for military service, exempt from conscription for military service in peacetime and credited to the reserve).
In some cases, the patient is assigned category G (a deferment of 6–12 months is given) and is offered surgery. After it is carried out, a re-examination occurs, and the functions of the joint are determined, as a result of which a category is assigned.
If surgical intervention is refused, category B is assigned, but in this case, the shoulder dislocation must be recorded by a doctor at least once every six months.
Why does the arm not rise up after a shoulder dislocation?
The cause of this pathology can be a rupture of the muscles or tendons of the rotator cuff, which make it possible to perform rotational movements in all directions. In this case, when the arm is moved upward at an angle of 70–120 degrees, the limb weakens and pain occurs.
In order to confirm the diagnosis, it is necessary to do an ultrasound, x-ray and MRI. Subsequently, the joint is immobilized and conservative treatment is prescribed (anti-inflammatory painkillers, corticosteroids).
If conservative treatment does not produce results within 2–3 months, the question of surgical intervention is raised.
Numbness of fingers after shoulder dislocation
In 20% of cases, shoulder dislocation is accompanied by nerve damage. Most often, paresis of the median nerve fibers occurs. The cause of neuropathy can also be arthrosis, arthritis or bursitis that develops as a result of injury. In this case, there is a loss of sensitivity in the fingers or certain areas of the skin.
If your fingers often go numb after an injury, you should consult a doctor and undergo an examination.. Drug stimulation of the neuromuscular system with Monofostamine injections and Bendazole tablets may be prescribed. Physiotherapeutic procedures, therapeutic exercises and massage are also prescribed. Nerve regeneration occurs very slowly, so the process of getting rid of numbness in the fingers after an injury is quite long.
If there is no improvement within six months, surgery is performed.
Immobilization for shoulder dislocation
Immediately after an injury, you should not try to correct the dislocation yourself, as this can lead to irreversible consequences. In order to carry out immobilization, you need to take a square piece of fabric and fold it in half.
The wide part of the scarf is placed over the shoulder, its ends are crossed under the armpit and tied tightly so that the bandage wraps around the shoulder and forearm (you can use any fabric that is at hand).
The disadvantages of this method include the fact that such a bandage cannot provide the appropriate level of fixation. This may cause the situation to worsen and cause tendon or muscle damage. Therefore, such a patient must be transported with caution.
To ensure that the joint is properly fixed, special bandages are used. Made from soft, breathable fabrics.
Often such models are provided with special clamps that allow the affected limb to be secured to the body. In addition, they allow you to relieve tension from the injured arm, thereby helping to quickly eliminate swelling and reduce the inflammatory process.
Depending on the patient's age and the severity of the injury, the restraint bandage will need to be worn for 2 to 6 weeks. For complex dislocations of the humerus, accompanied by damage to muscles, tendons and nerves, a Deso plaster cast can be applied for a period of one month.
The decision to mobilize the injured limb is made by the doctor after a visual examination and radiography. Only he can decide whether to apply a plaster cast to the patient or whether a fixing bandage is sufficient.
You can learn more about first aid for a dislocated shoulder.
If shoulder dislocation occurs more than 3 times, surgery is recommended to fix the affected joint.
How long does it take for a dislocated shoulder to heal?
Recovery from a shoulder dislocation in most cases depends on the patient. First of all, there must be a question about the duration of the immobilization period. If the patient is young and the injury is not too serious, the retaining bandage can be removed after 2 to 3 weeks. If a shoulder dislocation occurs in an elderly person, then fixation is carried out for 3 to 6 weeks.
The functions of the shoulder joint are fully restored within 3 months. In order to shorten this period, it is necessary to follow all the doctor’s recommendations, perform therapeutic exercises, massage and carry out physiotherapeutic procedures. In order to avoid re-dislocation of the shoulder, you need to avoid heavy physical labor for 6 months. In older people, rehabilitation may take a longer period, and pain may persist for six months after injury.
After the first dislocation, rehabilitation takes a longer period than with a repeated injury. If a shoulder dislocation occurs regularly, the pain may be minimal, and the affected joint may move back into place on its own. This is a fairly serious pathology requiring surgical intervention.
Sick leave and certificates for shoulder dislocation
Immediately after a dislocation of the shoulder joint, it is necessary to seek advice from a traumatologist, since an emergency doctor does not have the right to issue a document allowing the patient to stay at home.
The duration of sick leave depends on the severity of the injury, age and ability to work of the patient. It is the attending physician who, after the examination, decides what period is required for the patient’s rehabilitation. The maximum period for which sick leave is issued is 15 calendar days, after which the need for it must be confirmed. If the patient does not attend to this issue, then the sick leave is automatically closed and the employee becomes able to work.
Article publication date: 05/31/2016
Article updated date: 12/05/2018
Shoulder dislocation is an extremely painful condition in which the head of the humerus comes out of the socket, causing loss of contact between the articulating surfaces and disruption of the entire shoulder.
The mechanism of development of shoulder dislocation is similar to such pathology in other joints; The key difference between shoulder joint injuries is that they occur much more often, accounting for more than 50% of all diagnosed dislocations. This is explained by the complex anatomical structure of the joint and a large range of motion in different projections, which is why the shoulder is more likely to be injured.
The main causes of this pathology are various injuries, weakening of the capsular-ligamentous apparatus and diseases of both the joint itself and general diseases affecting large and small articular joints.
When a shoulder is dislocated, a person’s quality of life suffers greatly, as the injured arm practically ceases to function. Relapses are also possible, and repeated dislocations can occur not just once, but from 2 to 10 times a year. Repeated loss of the head of the bone from the glenoid cavity causes destruction of the elements of the shoulder joint - arthrosis or arthritis may occur.
The dislocation is successfully treated. A favorable prognosis after repositioning the head of the humerus bone in place largely depends on timely, qualified medical care, and whether such a pathology occurs in the patient again depends on the patient’s compliance with medical recommendations.
This pathology is dealt with by a traumatologist.
Types of pathology
| Gradation by category | Types of dislocations |
|---|---|
|
Regarding the time of acquisition |
Congenital |
|
Acquired |
|
|
Acquired dislocations are divided according to the causes of occurrence |
Traumatic (primary) |
|
Habitual (non-traumatic, resulting from insufficient strengthening of the shoulder tendons after a traumatic dislocation) |
|
|
Pathological (occurring against the background of tumors or any diseases) |
|
|
Voluntary (occurs spontaneously when performing everyday actions) |
|
|
By location of humeral head displacement |
Anterior (the head is shifted forward, going under the coracoid process of the scapula - subcoracoid dislocation, under the collarbone - subclavian) |
|
Inferior (downward displacement of the head of the bone) Rear (backward shift) |
In traumatological practice, in 75% of cases of the total number of all shoulder dislocations, anterior traumatic is diagnosed. In second place is the lower dislocation of the shoulder joint - it accounts for about 20% of cases.

Click on photo to enlarge
Common reasons
(if the table is not completely visible, scroll to the right)
| Causes | Specific pathologies or diseases |
|---|---|
|
Fracture of the glenoid cavity, head of the bone, coracoid and other processes of the scapula |
|
|
Fall on the outer side of an outstretched arm |
|
|
Congenital anomalies of development of the articular elements of the shoulder joint |
Insufficiently formed lower part of the glenoid cavity, rotator cuff weakness and other defects |
|
Stretching the joint capsule |
Monotonous daily repeated movements in the shoulder joint at the limit of its capabilities (typical of athletes, tennis players, swimmers) |
|
Generalized hypermobility is an abnormal increase in the range of motion in a joint due to weakening of the muscles and ligaments that fix it. Excessive mobility of the shoulder joint is typical for 10–15% of the planet's inhabitants |
|
|
Joint diseases |
Arthritis, arthrosis |
|
Systemic and other diseases |
Tuberculosis, osteomyelitis, osteodystrophy, osteochondropathy |
Repeated injuries to the shoulder lead to weakening of the ligaments, and as a result, the stability of the joint itself also weakens. Insufficient recovery of the rotator cuff muscles after a traumatic type of dislocation leads to another dislocation - a habitual one.
The repeated occurrence of this problem can be provoked by ordinary everyday movements: cleaning a house or apartment, washing floors, trying to put something on a high shelf, etc. Moreover, each repeated loss of the head of the humerus from the bed increasingly disrupts the stability of the joint, resulting in an interval between relapses are decreasing, and lesions are occurring more frequently.

Characteristic symptoms
The symptoms of a dislocated shoulder joint are in many ways similar to the symptoms of such damage to other joints.
Immediately after the humeral head leaves the articular bed, a sharp, severe pain occurs in the corresponding place. The arm droops, the shoulder becomes deformed. Any movement in the joint is impossible due to increased pain and disruption of its functioning. When trying to make a passive movement, springy resistance is felt.
A visually noticeable symptom is asymmetry of the shoulder joints. The articulation itself is deformed: angular, concave or sunken. When palpating, the doctor determines the protruding head of the bone that has emerged from the articular bed.
- An anterior dislocation is characterized by a downward and forward displacement of the head.
- For the anteroinferior - displacement to the anterior part of the axilla or down the coracoid process of the scapula. In this case, the person is forced to hold his hand in the most advantageous position: abducted and turned outward or bent.
- In the lower form of the pathology, the head is displaced into the armpit. A distinctive feature of a lower dislocation from others is the likelihood of numbness of the entire arm or certain parts (fingers or forearm) due to compression of the nerves located under the armpit. It is possible to immobilize muscles that were “connected” to the central nervous system by a pinched nerve.
- In a posterior dislocation, the head is displaced towards the scapula.
When the pathology recurs, the pain syndrome is usually moderate or mild. But the reduction of an old, repeatedly occurring dislocation becomes difficult due to the compaction of the articular capsule and the gradual filling of the cavity and nearby free areas with fibrous tissue (special connective tissue).
Other symptoms are swelling of the shoulder joint, a crawling sensation on the arm, pain not only in the area of the injury, but also along the pinched nerve.

Diagnostics
Diagnostic methods for dislocations of any joints are almost identical.
A traumatologist determines a dislocation of the shoulder joint based on visual examination, palpation, X-ray results in two projections (confirming the presence of pathology) and, if necessary, the results of computed tomography or magnetic resonance imaging.
If there is obvious damage to the blood vessels, consultation with a vascular surgeon is required; if a rupture or compression of the nerves is suspected, a consultation with a neurosurgeon is required.
First aid for a sprain
Completely avoid any movement of the injured limb.
Give the victim pain medication.
Apply ice or a cold compress to the affected area.
Make a splint from available materials to immobilize the arm and use a scarf, scarf or other object to secure the limb. Or, if possible, place a rolled-up towel under your armpit and secure the bent arm with bandages to your torso or to the shoulder girdle of your other arm.
Call an ambulance or immediately take the victim to the emergency room.
Basic treatment (3 stages)
Treatment takes place in three stages.
The first stage is reduction
Reduction can be closed (non-surgical) or open (surgical). Closed reduction of a fresh (several hours ago) shoulder dislocation is carried out under local anesthesia; for this, the affected area is injected with novocaine. One of the muscle relaxants is injected intramuscularly to relax the muscles, and in case of severe pain, a narcotic analgesic is administered. Old dislocation of the shoulder joint (more than a day) is eliminated under general anesthesia.
The most common options for realigning the shoulder joint are: the Dzhanelidze, Mukhin-Mota, Hippocrates, and Kocher methods. The traumatologist chooses which one to use depending on the type of injury.
Reduction of habitual, repeatedly occurring lesions or those that could not be eliminated by the closed method is performed surgically with fixation of the head of the humerus with special knitting needles or Mylar sutures in the glenoid cavity.
Symptomatic drug treatment at this stage consists of taking non-steroidal anti-inflammatory drugs and non-narcotic analgesics.
The second stage is temporary immobilization
Immobilization (immobilization) is necessary after reduction to secure the joint in the desired position, heal the capsule and prevent relapses. A special Deso bandage or splint is applied to the arm for about a month. As soon as the joint assumes a physiologically correct position, the symptoms of injury quickly disappear.

Deso bandage
It is important to follow the recommended period of wearing the Deso bandage, even if the swelling, pain and other symptoms of the disease have disappeared. If shoulder immobilization is stopped early, the joint capsule will not have time to heal, which will inevitably lead to habitual dislocation with injury to surrounding tissues.
The third stage – rehabilitation
A rehabilitation specialist is responsible for restoring the functions of the joint after immobilization. Physiotherapy (massage, electrical muscle stimulation) and exercise therapy help strengthen the ligaments and muscles of the shoulder.
Rehabilitation is divided into three periods:
The first 3 weeks are aimed at increasing muscle tone and activating their functions after immobilization.
The first 3 months are spent developing the joint and restoring its functionality.
Up to six months are allotted for complete restoration of the functioning of the shoulder joint.
The above stages of treatment are relevant for dislocations of any joints; there is a difference only in some nuances (for example, if the knee is affected, they do not use a Deso bandage for immobilization, but a bandage, side splint or other orthopedic device).
Summary
If a shoulder dislocation occurs, seek medical help immediately. The sooner you get to a traumatologist, the easier it will be for him to fix the problem.
After reduction, it is imperative to observe the recommended period of immobilization and rehabilitation, otherwise relapses of dislocation cannot be avoided, each of which will be accompanied by an increase in pathological changes in the articular elements.
Owner and responsible for the site and content: Afinogenov Alexey.
Read more, you will like:

Trauma can happen to anyone at unexpected times. Depending on the situation, any part of the body can be injured. When falling, a person tries to protect himself by putting his hands up to reduce the consequences. Shoulder dislocation is a fairly common injury in both adults and children. Such injuries can lead to a decrease in a person’s quality of life, which can subsequently affect his emotional background.
The shoulder joint is the most mobile joint in the human body, but in addition it is also the most vulnerable during injury. This joint is surrounded by a capsular-ligamentous apparatus, which at the time of heavy load does not sufficiently perform its protective functions. When receiving any injury, adults and children should be examined by a doctor to make a correct diagnosis.
 The following causes the development of such an injury:
The following causes the development of such an injury:
- features in the structure of the joint;
- injury;
- joint hypermobility;
- habitual joint tension when performing similar activities (swimming, gymnastics).
The listed reasons can influence separately or in combination.
The anatomical features in this case are dysplasia of the glenoid cavity of the scapula. This is due to the fact that the joint is not initially firmly fixed, so excessive impact on it can lead to traumatic damage. Joint hypermobility involves weakness of the ligaments and muscles that hold the joint in place.

This is, as a rule, a congenital feature of the musculoskeletal system and occurs quite often. But don’t be alarmed, not all people have this problem; this feature ends in dislocation of the shoulder joint.
Sport is one of the main reasons for the development of this disease. Constant training and stress on the joint can provoke such injuries. Performing monotonous movements for quite a long time, the ligaments are stretched, and they no longer perform their function so firmly. The very fact of injury and the presence of structural features of the shoulder joint increases the likelihood of a dislocation.

Photo: Symptoms of shoulder dislocation
It should be noted that the symptoms of an acute condition and habitual dislocation of the shoulder joint are generally the same, but there are a number of features that will be discussed below.
The main symptoms include:
- sharp pain in the shoulder joint and swelling;
- change in joint shape;
- fixed hand position;
- inability to make active and passive movements;
- change in limb length;
- decreased or impaired sensitivity in the joint area.
In most cases, these complaints arise as a result of active trauma. Some patients may develop a fever due to severe pain. The pain is usually intense, unbearable, and can lead to fainting. A person does not always immediately understand what happened. Trying to move the arm and perform minimal actions, they only worsen the clinical picture.
 If it speaks of a habitual dislocation of the shoulder joint, then it can form even in the absence of an active injury. Considering that the ligamentous apparatus is stretched, dislocation occurs when performing basic actions.
If it speaks of a habitual dislocation of the shoulder joint, then it can form even in the absence of an active injury. Considering that the ligamentous apparatus is stretched, dislocation occurs when performing basic actions.
If the neurovascular bundle is damaged, local circulation is disrupted and sensitivity changes. Sensitivity is impaired in the forearm and lower arm.
It should be noted that the symptoms of the condition differ in intensity and brightness depending on the individual characteristics of each person. When a diagnosis is made, a manipulation is performed such as reduction of the dislocation.
This is necessary because when an injury occurs, swelling of the soft tissues forms and if the dislocation is not reduced, the swelling will persist and the severity of the pain will increase. In addition to basic traumatological techniques, the patient must also be provided with psychological assistance.
 First aid for a dislocated shoulder should include:
First aid for a dislocated shoulder should include:
- fixation of the limb and application of cold;
- giving the patient a comfortable position;
- the need to relieve pain symptoms.
If a limb is damaged, it is necessary to record the time; in the future, this will help in choosing treatment tactics for the patient. The joint is fixed with a splint, bandages, or a scarf. It is necessary to firmly immobilize the injured arm to prevent additional displacement.
Cold must be applied; it will help prevent the development of severe swelling and relieve some pain. For pain, analgesics with an anti-inflammatory effect are used. First aid for a dislocated shoulder joint can be provided by a person without special education.
It is necessary to reduce a first-time dislocation in a hospital after additional examination. This must be done as quickly as possible so that the recovery period is more effective. To confirm the diagnosis, it is enough to conduct an X-ray examination, which can clearly determine the violation of the integrity of the joint.
 Habitual dislocation of the shoulder joint; features of the clinical picture
Habitual dislocation of the shoulder joint; features of the clinical picture
A dislocation that recurs three months after the initial dislocation is considered habitual. Over time, objectively, such patients experience a decrease in muscle volume in the shoulder area.
Moderate pain is present not only at rest, but also upon palpation of the shoulder area. The pain with a habitual dislocation of the shoulder joint is not so intense, the body temperature does not rise and the patient immediately begins to take the necessary actions.
The reasons for the formation of habitual dislocation are as follows:
- muscle rupture;
- sprain or rupture of joint ligaments;
- any sudden movement of the hand;
- incorrect treatment of the primary injury (most often not follow-up treatment);
- re-injury and much more.

With fairly frequent relapses of the disease, the causes of dislocation become less and less significant, which aggravates and prolongs the process of restoring normal functioning of the joint. Reduction of a dislocation is easy, and patients can often perform it on their own.
This disease reduces a person’s quality of life, primarily due to the fact that restrictions on physical activity have to be observed so as not to provoke an exacerbation of the condition. In addition, constant pain and discomfort leads to decreased mood and performance.
Treatment for such conditions is usually surgical. This is necessary because conservative therapy is not very effective and does not bring relief to the patient. Plastic surgery of the capsular-ligamentous apparatus is performed, which is aimed at strengthening and fixing the joint in the correct position.
There are several methods of surgical treatment, each is selected individually depending on the nature and neglect of the process. After such treatment, a recovery and rehabilitation period is required. Treatment must be comprehensive and continuous, then the desired result can be achieved.
Treatment
 Treatment of a dislocated shoulder joint begins immediately, from the moment first aid is provided to the patient. The sooner these activities begin, the more productive the result will be. The main type of treatment for this condition is reduction of the dislocation.
Treatment of a dislocated shoulder joint begins immediately, from the moment first aid is provided to the patient. The sooner these activities begin, the more productive the result will be. The main type of treatment for this condition is reduction of the dislocation.
The manipulation is not simple and requires professional skill. Doctors who perform these procedures are orthopedic traumatologists or surgeons.
Reduction of a first-time dislocation is the most labor-intensive procedure. Before proceeding with the manipulation, it is necessary to anesthetize the patient (local anesthesia or anesthesia, it is decided individually); in some cases, for complex dislocations, muscle relaxants are used to further relax the muscles in the damaged area.
It will be effective for joint pain.
The following reduction techniques are distinguished:
After the manipulation, drug therapy is necessarily prescribed, which will be aimed at relieving swelling, inflammation, improving blood circulation in the joint and muscles, vitamin therapy, and reducing pain.
Treatment of a dislocated shoulder joint after reduction includes fixation of the limb and a rehabilitation course. Physiotherapeutic treatment is an addition to primary therapy.
Surgeries for dislocation of the shoulder joint are performed to treat habitual dislocation or new dislocation, when conservative reduction is not possible.

Photo: X-ray of a dislocated shoulder joint
Surgical treatment can take place:
- on the joint capsule;
- on ligaments;
- on the muscles;
- on the bones;
- or be a combination.
Surgical reduction of a dislocation is considered a simple procedure. It is based on opening the joint capsule, restoring the correct relationship of bones and suturing damaged tissues. Much more painstaking and delicate surgery is used to treat habitual joint dislocation. This is due to the fact that over time, with constant load and trauma, the joint changes.
Fibrous cords and growths form. Muscles and ligaments weaken and stop functioning normally. Taking this into account, during the operation the doctor “cleanses” the joint to improve the contact of the articular surfaces.
The main goal of the operation for habitual shoulder dislocation is to create a strong capsular frame that will prevent damage to the joint. 
In most cases, treatment involves combined operations, which include effects on ligaments, muscles, bones and surrounding tissues. It is rare to resort to isolated treatment of any one structure. Immobilization of the limb is mandatory after such treatment. The period is determined individually, but, as a rule, it is not less than three weeks.
If, after the reduction procedure, the patient notes persistent swelling of the upper limb and its increase, feels numbness and weakness in the arm, the pain does not go away, but rather intensifies every day, it is necessary to inform the doctor about this, since these may be signs of complications of this disease.
Some patients find surgical treatment quite difficult, so support from psychologists or psychotherapists can ease the postoperative period and speed up recovery.
Recovery and rehabilitation after treatment
Every patient must understand that after reduction of a dislocation it is necessary to carry out rehabilitation and observe the recovery period. The entire course lasts at least six months. Rehabilitation is necessary to develop the joint after injury.
If these procedures are not completed in full, the patient may experience the possibility that the dislocation may occur again, and then the disease will become chronic. Rehabilitation for shoulder dislocation is developed individually for each patient. The course necessarily includes the development of:
- ligaments and muscles;
- restoration of range of motion;
- prevention of disease relapse.
The duration of the recovery period depends on the severity of the condition, the age of the patient, and the neglect of the process.
It should be noted that after the procedure the patient does not immediately begin warm-up exercises. The first week is aimed at creating maximum rest for the fixed limb. This is necessary so that maximum fusion of all damaged tissues occurs, to exclude secondary inflammation.
 During the first postoperative week, the patient takes drug therapy, volumetric movements in the joint are limited, and small exercises in the hands and fingers are allowed to improve blood circulation in the hand.
During the first postoperative week, the patient takes drug therapy, volumetric movements in the joint are limited, and small exercises in the hands and fingers are allowed to improve blood circulation in the hand.
The second stage of recovery begins in the second week and lasts up to four weeks. Here the patient is allowed to perform smooth, measured movements in the arm and joint. After the manipulation, cold is applied to reduce pain. Sharp and complex combined movements are prohibited, as this can provoke a new dislocation.
The third period of recovery lasts up to six months. The main task is to restore the full range of motion in the joint and stop the inflammatory process. Rehabilitation, in addition to gymnastic techniques, should include massage and physiotherapeutic procedures.
What makes physiotherapy convenient is that it affects joint structures without force. The main physiotherapeutic procedures include:
- electrophoresis with novocaine;
- magnetic therapy and laser;
- UHF and UVT;
- phonophoresis;
- electrical stimulation.

Thanks to these techniques, metabolic processes are improved, the body's immune response is increased, barrier mechanisms are activated, and recovery is accelerated. The listed techniques can be used alternately or together.
The main point in rehabilitation for a dislocated shoulder joint is exercise therapy. Therapeutic physical education is carried out under the supervision of an instructor, who describes step by step what tasks need to be carried out. Exercise therapy for a dislocated shoulder joint is aimed at restoring muscle strength and at the same time relieving muscle tension. With well-chosen exercises, the load on the joint is gradually increased, increasing the strength of the tasks.
Gymnastics in the early stages helps to normalize muscle functions, then leads to the restoration of joint functionality. After immobilization has been removed, physical therapy exercises are aimed at reducing muscle contractures and increasing the endurance of muscle tissue. It should be noted that tasks are performed with a sick hand and a healthy one.
The following exercises are mainly used:
- raising your arms to the sides;
- flexion and extension in the elbow joint and hands;
- raising your arms up;
- circular movements;
- putting your hands behind your back.
We must not forget that in the first days of rehabilitation therapy, not all procedures will be performed in full, but systematic exercises help expand the range of active and passive movements. Exercise therapy for a dislocated shoulder joint is first carried out in a lightweight version, then, with good load tolerance, sports equipment can be added. Most often they use dumbbells, balls, and a stick. The duration of classes starts from 10-15 minutes, gradually the time interval increases.
- infraspinatus - located on the body of the scapula, as you might guess from the name, under its axis and is responsible for supination of the shoulder;
- supraspinatus - located above the axis, is involved in abducting the shoulder from the body. The first 45 degrees of abduction are performed primarily by the supraspinatus muscle;
- subscapular - located on the anterior surface of the body of the scapula (between the scapula and the chest) and is responsible for performing supination of the head of the humerus;
- large round - runs from the lower pole of the scapula to the head of the humerus, woven into the capsule by a tendon. Together with the infraspinatus muscle it performs pronation of the shoulder.
- the biceps flexes the shoulder, bringing the body of the humerus 90 degrees to the upper shoulder girdle;
- the triceps, together with the posterior head of the deltoid muscle, extends the shoulder, moving the body of the humerus back relative to the body of the scapula;
- pectoralis major and minor muscles - responsible for bringing the humerus bones towards each other;
- The latissimus dorsi muscles provide downward movement of the bodies of the humeral bones in the frontal plane.
- the scapula axis is the point of origin of the posterior portion of the deltoid muscle;
- acromion - attachment point of the middle portion of the deltoid muscle;
- The acromial end of the clavicle is the attachment point of the anterior portion of the deltoid muscle.
The shoulder joint is the most mobile in the human body. All types of movements are possible in it: flexion-extension, abduction-adduction, supination-pronation, rotation. The price for such freedom of movement is the significant “fragility” of this joint. This article will talk about the most common injury that awaits athletes who systematically overload their shoulder joints. This is a dislocated shoulder. In addition to the injury itself, we will touch upon issues of anatomy, biomechanics, first aid and, most importantly, preventive measures.
Anatomy of the shoulder joint
The shoulder joint is directly formed by the head of the humerus and the glenoid cavity of the scapula. The articular surfaces of the designated bones do not have absolute congruence. Simply put, they are not perfectly adjacent to each other. This moment is compensated by a large formation called the articular labrum. This is a cartilaginous body adjacent, on the one hand, to the articular cavity of the scapula, on the other, to the head of the humerus. The area of the articular lip is much larger than that of the articular surface of the scapula, which ensures greater adherence of the articulating surfaces within the joint. The head of the humerus and the glenoid cavity of the scapula are covered with hyaline cartilage.
Joint capsule and clavicle
The described structure is covered on top by a thin articular capsule. It is a sheet of connective tissue that covers the anatomical neck of the humerus on one side and the entire circumference of the glenoid cavity of the scapula on the other. Fibers of the coracobrachial ligament, the tendons of the muscles that form the so-called rotator cuff, are also woven into the tissue of the capsule. These include the infraspinatus, supraspinatus, teres major and subscapularis muscles.
The listed elements strengthen the shoulder capsule. The muscles that form the rotator cuff provide a certain range of motion (read more about this below). Taken together, this formation limits the immediate joint cavity.
The clavicle also plays an important functional role in the structure of the shoulder joint. Its distal end is attached to the acromion or acromial process of the scapula. When the shoulder is abducted above an angle of 90 degrees, further movement occurs due to the mutual movement of the clavicle, the lower pole of the scapula and the chest. Looking ahead, we will also say that the main muscle serving the shoulder joint - the deltoid - is attached to the described anatomical complex.

Rotator muscles
The condition of the muscles surrounding it is important for the health of the joint. (this statement applies to all joints of the human body, not just the shoulder ones). Let us repeat that the muscles serving the shoulder joint are located, so to speak, in two layers. The deep muscles include the already mentioned muscles - rotators:
Moving muscles
The tendons of the biceps and triceps brachii muscles pass over the joint capsule. Since they extend over the head of the humerus, attaching to the acromion process of the scapula, these muscles also provide certain movements in the shoulder joint:
It should be mentioned that the pectoralis major and minor muscles and the latissimus dorsi muscles are also attached to the articular tubercles of the humerus, providing the corresponding movements:
The deltoid muscle is directly responsible for movements in the shoulder joint. It has the following attachment points:
Each portion, in fact, performs a different function, but balanced movements in the shoulder joint require the coordinated work of all three “bundles”. This is emphasized by the fact that all three delta bundles converge into a single tendon, attached to the deltoid tuberosity of the humerus.
The large volume of the listed muscles provides an appropriate range of movements. However, practically they are the “base” of the joint. The shoulder does not have a reliable bone structure, which is why during sports activities, especially when performing amplitude movements, the shoulder joint is injured.

Mechanism of injury
A shoulder dislocation is a displacement of the head of the humerus relative to the glenoid cavity of the scapula. There are several types of shoulder dislocation based on the direction of displacement.
Anterior dislocation
This type of injury occurs most easily, since it is the posterior pole of the humeral capsule that is least strengthened by tendons and ligaments. In addition, the posterior portion of the head of the deltoid muscle must provide stability. However, it is not sufficiently developed in the vast majority of ordinary people, and athletes are no exception.
This injury can occur under the influence of a jerking effect on a limb - when practicing martial arts, performing elements on the rings, or on the uneven bars, the starting point for entering a handstand. An anterior dislocation is also possible due to a blow to the shoulder joint - when practicing striking martial arts (boxing, MMA, karate), or when landing after performing a jumping element (workout, parkour).
Posterior dislocation
Posterior shoulder dislocation and with does not occur as often as the front one, but, nevertheless, quite often in percentage terms. In this case, the head of the humerus moves to the back of the glenoid cavity of the scapula. As you might guess, such a displacement of the humeral head occurs when the anterior pole of the shoulder joint capsule is injured. Most often, the shoulder is in a flexed position, with the arms extended in front of the body. The impact occurs on the distal part of the arm. In other words, in the palm of your hand. Such an impact is possible when falling on outstretched arms, for example, with insufficient technical performance. Or when the weight of the barbell is incorrectly distributed when performing a bench press.

Lower dislocation
With an inferior dislocation, the head of the humerus is displaced under the glenoid cavity of the scapula. This type of injury is not common and occurs when the arm is raised up. Such an injury is possible when performing the “flag” exercise, when performing walking on hands, snatch and push. Snatch and push, in this case, are the most traumatic, since the shoulders are in an anatomically unfavorable position, and the load is vertical.
Habitual dislocation
There are other types of shoulder dislocations, but they are essentially combinations of the types of injury described above.
The most unpleasant consequence of a shoulder dislocation is its chronicity - the formation of a habitual dislocation. This condition is characterized by the fact that any minimal impact on a previously affected joint is enough to cause a full-fledged dislocation. Most often, this pathology develops due to improper treatment of a primary shoulder dislocation.
Signs and symptoms of a dislocation
The following unpleasant symptoms indicate an injury to the shoulder joint, namely a dislocation:
- Sharp pain in the area of the damaged joint, accompanied by a kind of “wet crunch”.
- Inability to make active movement in any of the axes of mobility of the shoulder joint.
- Characteristic displacement of the head of the humerus. In the deltoid region, the acromial process of the clavicle is determined, under it there is a “depression”. (With a lower dislocation, the arm remains raised upward, the head of the humerus can be felt in the chest area, under the armpit). The area itself, compared to a healthy one, looks “sunken”. In this case, the affected limb becomes relatively longer.
- Swelling of the affected joint area. Develops due to traumatic damage to the vessels surrounding the joint area. The spilled blood permeates the soft tissues, sometimes forming a fairly large hematoma, which brings additional pain. Moreover, you will not see “blue discoloration” of the deltoid region immediately after injury; subcutaneous vessels are damaged extremely rarely, and a visible hematoma is characteristic only of direct injury to these vessels.

First aid for a dislocated shoulder
Don't try to straighten your shoulder yourself!!! In no case! Inept attempts at self-reduction of the shoulder lead to injuries to the neurovascular bundle and serious ruptures of the shoulder capsule!
First, you need to fix the limb, ensuring its maximum rest and limited mobility. If there is a painkiller (analgin, ibuprofen or diclofenac and the like), it is necessary to give the medicine to the victim to reduce the severity of the pain syndrome.
If there is ice, snow, frozen dumplings, or vegetables, it is necessary to apply an existing cold source to the damaged area. The entire deltoid region should be in the “cooling” zone. This way you will reduce post-traumatic swelling in the joint cavity.
Next, you need to immediately deliver the victim to a medical facility where there is a traumatologist and an X-ray machine. Before reducing the dislocation, it is necessary to take an X-ray of the shoulder joint to exclude a fracture of the body of the humerus and scapula.
Treatment of dislocation
As for how to treat a dislocated shoulder, we will give only a few general tips, since self-medication in this case can be very dangerous. The treatment process includes several stages:
- reduction of the dislocation by a qualified traumatologist. Better - under local anesthesia. Ideally, under anesthesia. Pain relief provides relaxation to muscles that spasm in response to injury. Thus, the reduction will be quick and painless.
- immobilization and ensuring complete immobility of the shoulder joint. The period of immobilization is 1-.5 months. During this period we try to achieve maximum healing of the shoulder capsule. For this purpose, during this period, a variety of physical therapy is prescribed to help improve blood circulation in the affected joint.
- rehabilitation.
We will talk about the rehabilitation stage for a shoulder dislocation in more detail below.

Rehabilitation
It is necessary to gradually expand the range of movements immediately after removing immobilization. Despite the fact that the connective tissues have grown together, during immobilization the muscles have weakened and cannot provide proper stability to the joint.
First stage of recovery
In the first three weeks after removing the fixing bandage, kinesio tape can be a reliable help, activating the deltoid muscle and thereby increasing the stability of the joint. During this same period, all possible presses and deadlifts should be eliminated. The remaining exercises available are:
- Straight arm abduction to the side. The body is fixed in a standing position straight. The shoulder blades are brought together, the shoulders are separated. Very slowly and under control, we move our arm out to the side at an angle of no more than 90 degrees. We also slowly return it to its original position.
- P ronation-supination of the shoulder. The elbow is pressed to the body, the arm is bent at the elbow joint at 90 degrees. The humerus stands still, only the forearm moves. We alternately bring and abduct it, with dumbbells clamped in the hands, left and right. The amplitude is minimal. The exercise is performed until a feeling of warmth, or even heat, appears in the inside of the shoulder joint.
- WITH bending the arms in a machine that eliminates traction of the injured arm. Such, for example, is a block exercise machine with a built-in Scott bench.
- R when bending the arms in a machine that simulates the French bench press, the humerus in relation to the body should not be placed at an angle of more than 90 degrees.
The weight of the weights is minimal; when performing them, you need to concentrate on the muscle sense. Barbells and dumbbells of moderate and heavy weight are completely prohibited at this moment.
Second phase
Three weeks after removing immobilization, you can include front raises and bent over flyes to engage the anterior and posterior portions of the deltoid muscle, respectively.
We begin to perform side flyes in two versions: with small dumbbells and extremely clean technique - to strengthen the supraspinatus muscle, and with slightly heavier dumbbells (preferably in a machine, but it may not be available in your gym) to target the middle portion of the deltoid muscle.
Thus, you need to train for another three weeks. And only after this period has passed, you can carefully return to your usual training regimen, gradually including pressing and pulling movements into the training program. Better - in simulators, with moderate or even light weights.
Third stage
After the four-week stage, you can move on to working with free weights. It’s better to start with a barbell, and only after that move on to working with kettlebells and dumbbells. Once you have mastered the movements with them, you can start working with your own weight again.
Prevention of shoulder dislocation involves systematically strengthening the rotator cuff muscles using the exercises described in the first stage of rehabilitation and working with each muscle bundle separately. Particular attention should be paid to the posterior portion of the deltoid muscle, which is responsible for the stability of the posterior pole of the shoulder joint capsule.
You should never start training deltoids with heavy weights and bench press exercises. As a warm-up, it is very useful to pump up each bundle individually and perform exercises for the rotator cuff.
Injurious exercises
As is not difficult to understand from what was written above, the most traumatic exercises in CrossFit are gymnastic elements performed on rings and parallel bars, snatch, clean and jerk and exercises leading to them, walking and handstands.
However, not a single exercise will harm you if you approach your exercises wisely and in a balanced manner. Avoid one-sided loads, develop your body harmoniously and be healthy!
The shoulder joints are the most mobile in the entire body. For a large number of varied movements of the shoulders, we pay with high injuries to the shoulder joint. It is shoulder dislocation that accounts for more than half of all dislocations and about 3% of all injuries. Its treatment and subsequent rehabilitation depend on many factors: the type of dislocation, how long ago the injury was received, the presence of complications, and the cause. Such shoulder damage is most often reversible: it is completely restored with proper treatment.
Shulepin Ivan Vladimirovich, traumatologist-orthopedist, highest qualification category
Total work experience over 25 years. In 1994 he graduated from the Moscow Institute of Medical and Social Rehabilitation, in 1997 he completed a residency in the specialty “Traumatology and Orthopedics” at the Central Research Institute of Traumatology and Orthopedics named after. N.N. Prifova.

The shoulder joint itself consists of three parts:
- articular head of the humerus;
- articular cavity of the clavicle;
- glenoid cavity of the scapula.
The cavity of the clavicle has no connection with the humerus, but has an impact on its functioning. Between the head of the humerus and the socket of the scapula there is an articular lip, which additionally holds the joint and maintains high mobility. The shoulder joint contains several bundles of articular ligaments, groups of muscles that provide great stability.
The mechanism of injury is excess of physiological amplitude due to indirect trauma. The joint capsule is destroyed, and the head of the humerus falls out. Sometimes there are fractures, damage to muscles and tendons.
Causes of shoulder dislocation
This injury is the most common of all injuries to the shoulder joint. Causes of dislocation include:

- injury (strong blow to the shoulder, fall on the arm);
- frequent muscle and tendon strains shoulders (found in athletes);
- identical hand movements which are often repeated (more often observed in athletes);
- congenital hypermobility– “joint hypermobility” (occurs in approximately 12% of people);
- abnormal structure of the scapula(small scapular cavity).
A dislocated shoulder in itself does not pose a serious threat to a person's health. But getting a second injury (habitual shoulder dislocation) within six months after the first injury to the shoulder joint is very high. This does not require strong impact on the site of the previous damage. The reason lies in improper reduction of the shoulder dislocation, treatment, or injury associated with severe rupture of the joint box.
Characteristics of types of shoulder dislocations
Depending on various factors, there are several classifications of shoulder dislocations. Based on the presence of traumatic effects, they distinguish between traumatic (cause – injury) or non-traumatic(habitual) dislocation. Non-traumatic shoulder injury can be chronic (pathological) or voluntary. There is a division of shoulder dislocations into congenital (improper structure of the scapular cavity, hypermobility of the joints) and acquired.
Depending on the type of injury, dislocations can be uncomplicated or complicated (dislocation with bone fracture (fracture dislocation), with damage to the skin and tissue around the joint (open dislocation), with damage to tendons, nerves and blood vessels). Based on the time that has passed since the injury, dislocations are divided into fresh (the first three days), stale (up to five days), old (more than 20 days have passed).
Shoulder subluxation is a common injury that occurs in children and the elderly. It has no complications, but can recur if not properly treated. If the injury occurs for the first time, it is called a primary dislocation. After such damage, the tendon and the joint itself lose their original strength, and the risk of re-injury increases.

By the direction in which the articular head goes, how the articular surfaces diverge, they distinguish front, bottom and posterior shoulder dislocation.
Anterior dislocation
The most common type of such injury, more than 75% of shoulder dislocations (up to 90%) are anterior dislocations. It has two varieties: subcoracoid and subclavian. In the first case, the head of the bone falls out of the articular capsule and extends beyond the process of the scapula, called the coracoid. In a subclavian dislocation, the articular head moves even further and extends beyond the collarbone. With such an injury, serious complications are possible (rupture of the joint capsule, damage to soft tissues). The shoulder looks to the side.
Lower dislocation
An infrequent type of dislocation (from 8% to 24%). The lower dislocation is called axillary. Here the head of the humerus goes down relative to the glenoid cavity of the scapula. The victim cannot lower his arm; it is moved away from the body.
Posterior dislocation
Posterior shoulder dislocation is very rare (up to 2% of cases). It is observed when a person falls on his outstretched arm. The articular head goes simultaneously to the back and head. Often with a posterior dislocation, ligaments, tendons, and the articular labrum connecting the socket of the scapula and the head of the humerus bone are torn.
Symptoms of shoulder dislocation

With the variety of types of dislocations, the symptoms of such an injury are similar:
- sharp and severe pain in the area of injury (shoulder, arm, scapula, collarbone), worsening when trying to move the arm;
- the appearance of swelling in the shoulder joint;
- traffic restrictions(the victim can make a very small number of movements, often springy due to protective contraction of muscles and tension of ligaments and tendons; numbness of the hands is possible if the nerve is damaged);
- visible deformation shoulders (the shoulders are asymmetrical, the damaged side looks angular).
Signs of a complicated dislocation can be recognized by Bankart damage(increased pain), a characteristic crunch that accompanies a bone fracture, weak palpation of the pulse on the radial artery in case of vascular damage, numbness of the hand in case of nerve damage.
Diagnostics

The main symptoms by which a traumatologist determines the type of injury received are described above. Professional examination by a doctor occurs in the form of careful and careful palpation to establish the location of parts of the joint, determine its mobility, as well as a conversation with the victim. To clarify the presence/absence of complications, the doctor checks the pulse, palpates the skin, and checks the mobility of the fingers.
To clarify the diagnosis and select the most competent treatment, use X-ray and magnetic resonance imaging.
Shoulder joint treatment

After receiving an injury, you should immediately call an ambulance or go to the emergency room yourself. As first aid for someone who has suffered a sprain, you need to apply cold to the injury site, ensure peace and do not move the injured arm. If possible put a bandage on your hand, to immobilize the damaged joint as much as possible.
To reduce pain you need give painkillers.
You cannot straighten the shoulder on your own until the ambulance arrives.
You can aggravate the situation, damage surrounding tissues, and damage nerves and blood vessels. If there is an open wound, you need to treat it with an antiseptic and apply a bandage.
Next, depending on the situation, the doctor selects a treatment and recovery regimen. All methods are divided into surgical and non-surgical. Only a doctor can determine which one is suitable in a particular case.
Closed reduction of dislocation
You need to move the shoulder joint back into place as quickly as possible. To do this, local anesthesia or general anesthesia must be used: they are used for pain relief and muscle relaxation. There are several methods of reduction:
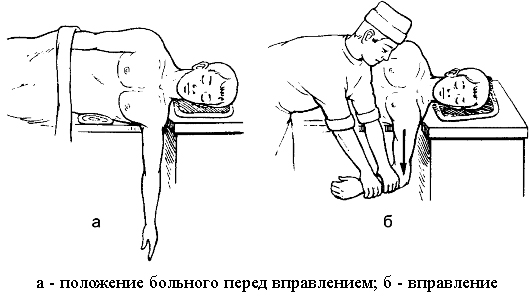
- according to Dzhanelidze;
- according to Kocher;
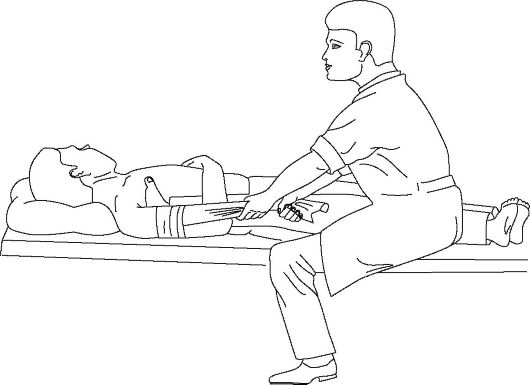
- according to Hippocrates;

- according to Mukhin-Mot and others.
After reduction, the pain decreases significantly. Subluxation of the shoulder joint without complications can be reduced without the use of anesthesia. You need to check the success of this manipulation using an x-ray. Then the doctor prescribes painkillers and applies a bandage or special fixation of the shoulder with abduction of the arm.
Even if there is no pain, you need to wear it for at least 3 weeks.
Surgery
This treatment method is often used for repeated habitual dislocations, when surgery is unavoidable. If a second dislocation occurs, it will happen again until the cause of the pathological condition of the shoulder joint is eliminated.
Dislocation of the ACJ (acromio-clavicular joint), often found among athletes, requires only surgical treatment, since such an injury causes ligament rupture.
When eliminating habitual shoulder dislocations, the surgeon pursues such goals as strengthening the ligaments and tendons, and correct alignment of the glenoid cavity and the head of the humerus. There are several types of operations to correct this type of dislocation:
- Turner operation(removal of an elliptical flap of the articular capsule, suturing the capsule; advantage - small scar, short recovery period);
- Putti operation (more traumatic, necessary in the presence of complications; the capsule is sutured; does not require a large number of instruments; minus - long recovery period, large T-shaped scar);
- Boychev's operation(similar to Putti’s operation; a triangular fragment is removed before suturing);
- Bankart operation(not so widespread due to the use of special devices (arthroscope); the goal is to create a new labrum; has a short recovery period; considered the gold standard in the treatment of dislocations).
The doctor’s choice of type of operation depends on the presence/absence of complications, special instruments, and the age of the victim.
The recovery period after such an operation lasts up to six weeks.
After surgery, a brace, a complex device for maximum immobilization and support, is used on the affected shoulder and arm.
Physiotherapy
The use of physiotherapeutic procedures is possible in the presence of a fixing bandage on the shoulder and after its removal. The goal of physical therapy is to reduce tissue swelling, relieve pain in the damaged area, restore good local blood flow and mobility of nearby muscles. They are aimed at restoring the damaged shoulder joint and its functions. Basic physiotherapeutic procedures:

- magnetic therapy (high and low intensity);
- electrophoresis (to accelerate the absorption of drugs);
- diadynamic therapy;
- amplipulse therapy;
- infrared irradiation;
- massotherapy;
- paraffin therapy;
- alcohol compress;
- local cryotherapy (low temperature exposure).
The main contraindications are purulent wounds, kidney and blood diseases, malignant tumors, bleeding, heart disease (heart attack), the presence of pacemakers, infectious diseases, tuberculosis. Some procedures have restrictions such as pregnancy, children under 5 years of age, and a tendency to develop blood clots.
They help shorten the rehabilitation period and reduce the severity of symptoms without medications. But their use should be agreed with the attending physician, you cannot assign them to yourself. Physiotherapy procedures do not replace joint realignment or surgical intervention.
Exercises after a sprain
Immediately after reduction and application of an immobilizing bandage, as well as approval from the doctor (for uncomplicated dislocations), you can begin a course of exercise therapy. Exercises after a sprain in the first weeks they are passive(performed with the help of a doctor or another healthy hand). Gradually you need to perform the exercises more actively. The first training should begin with flexion/extension and rotation of the hand, clenching the fingers into a fist, and static tension of the shoulder muscles.
A month after the injury and removal of the bandage or fixing bandage, you need to use the joint itself, moving your shoulders forward/backward at a slow pace several times during the day. This exercise helps restore the ligamentous apparatus, the function of the joint itself.
Once the bandage is removed, the importance of exercise increases. You shouldn't start playing sports right away. A properly selected course of exercise therapy helps to quickly strengthen damaged ligaments, strengthen the muscles around the joint, and stabilize the joint itself. The amplitude of movements should be increased gradually, and then include expanders, weights, and rubber bands. In the beginning, you should do the exercises under the guidance of a doctor, and then at home. After exercising, apply a cold compress to the injured area to relieve pain.
By performing simple exercises, you will speed up your recovery after a shoulder injury.
Treatment for repeated dislocations
If the dislocation occurs again, the doctor will prescribe surgical restoration of the joint capsule. Other methods will not be able to completely eliminate such injury in the future.
The operation can restore the function of the ligaments and the capsule itself. Therefore, the risk of injury recurrence is minimized. Particular attention should be paid to therapeutic exercises: it will help strengthen the joint, ligaments and muscle frame. Strong muscles reduce the likelihood of recurrent dislocations.
Rehabilitation and complications
The rehabilitation period after a dislocation consists of three stages, during which the method of treatment, physiotherapeutic procedures, and exercise therapy change.
At the first stage, lasting up to 21 days, any movements of the shoulder joint are limited. Drug therapy, a cold compress to relieve swelling, exercise therapy in the form of wrist movements, and static muscle tension are used. Physiotherapy at this stage should be aimed at relieving pain and swelling.
It is important to remember that prolonged restriction of movement for the elderly is dangerous due to the high risk of muscle atrophy. Therefore, their immobilizing bandage is removed earlier.
The second stage of rehabilitation begins after removing the fixing bandage.
It begins 4-6 weeks after injury and lasts up to 3 months.
Here the main role is played by special exercises that help restore the shoulder joint.
Complete restoration of the functionality of the joint occurs in the third stage.
It usually lasts up to six months. In older people, the period can last up to a year.
Complications after a shoulder dislocation include repeated dislocations (habitual), bone fractures, damage to nerves and blood vessels, and rupture of the labrum.
Dislocation of the shoulder joint, the most mobile joint in the body, is a common occurrence. To avoid it, you need to follow safety precautions when playing sports and physical labor. If injury cannot be avoided, you need to complete the entire course of treatment and follow the doctor’s instructions in order to further reduce the risk of re-injury.
How does a shoulder dislocation occur and what to do in this case?