Elastic ligaments in a child. The child's joints are weak. Nutrition for joints
Text: Elena Baburova, consultant - Sergey Vasiliev, pediatrician, doctor of the highest category
You can get a free consultation with pediatrician Sergei Vasiliev right now!
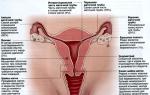
Probably, man looked at all technical inventions from nature. So our joints are like hinges when one bone slides in relation to another. For better gliding, they are created smooth and well adjusted to each other and, like machine oil, are lubricated with intra-articular (synovial) fluid. The bones are covered on top with articular cartilage, which gives external integrity to the entire structure and prevents joint fluid from leaking out. Inside this capsule, a joint cavity is formed, where fluid circulates. For strength, the joints are reinforced with ligaments that are woven into the joint capsule. Where by nature the bones do not fit each other perfectly, and also where the loads on the articular surfaces are high, nature has invented spacers - menisci.
So why do joints crack?
Joints crack: where does this sound come from?
Don't worry, the joint won't break. Scientists believe that joints crack due to the accumulation of gas bubbles in the synovial fluid. This liquid contains oxygen, nitrogen and carbon dioxide. Therefore, in those moments when the joint capsule is overstretched or a sudden movement is made, the gases collect in bubbles and then burst, accompanying this process with popping sounds.
Joints crack: looking for the cause
There are many reasons why joints crack, but most often it is not a disease and treatment is not required.
1. Underdevelopment of the ligamentous apparatus- connective tissue in children is not as dense as in adults and is more elastic, and the muscular system is less developed. Therefore, as a child grows older, his joints crack less and less often.
2. Connective tissue dysplasia. In some children, parents note “weak joints”: dislocations often occur, and the medical record contains diagnoses such as “scoliosis”, “mitral valve prolapse”, “myopia”, “flat feet”. The main cause of dysplasia is a structural change in collagen, as well as a deficiency of the components from which connective tissue is built. Joints crack due to the fact that the articular ligaments are stretched and the joints become loose, as a result, some elements of the cartilaginous surfaces come into contact. The disease is hereditary.
3. Decreased secretion function of the periarticular bursa. A lack of intra-articular (synovial) fluid impairs gliding and causes clicking and creaking.
4. Joint inflammation (arthritis) leads to the fact that a person’s cartilage tissue first changes, separations, cracks appear, and the cartilage tissue becomes thinner. Then these changes affect the bone: it becomes covered with growths, compactions, spines, and subsequently it becomes deformed and curved. Deformation of the articular surface leads to cracking joints, joint stiffness, swelling and severe pain even at rest.
There are 230 joints in the adult body. And the kids have even more! According to various sources, up to 350! With age, some joints simply grow together.
What to do if your child has cracking joints?
Show some common sense. If the crunching of your child’s joints bothers you, but nothing hurts your baby, you shouldn’t worry and take your child to the doctors. In most cases, crunching sounds that alarm you indicate that the child is growing up and his musculoskeletal system is developing.
Show attentiveness and vigilance. If the crunch is loud, one-sided, the joint swells, the baby complains of discomfort or even pain, you should immediately consult the child with an orthopedist. Get the necessary tests to rule out arthritis.
Crackling joints: is prevention possible?
If the doctor believes that the crunch is caused by joint hypermobility due to connective tissue dysplasia, you need to approach this issue very carefully. The fact is that such diseases can end arthrosis in adulthood.
What should you provide to your child if his joints are cracking?
Moderate physical activity. Discuss with the doctor whether it might be better for your child to attend a treatment group during physical education classes? You can’t avoid physical activity; you need to choose it correctly. Such kids should not engage in sports dancing and hockey. Swimming and cycling are just what you need. But long walking and carrying heavy objects can only do harm.
With age, joints become more rigid (stiff), so the older a child gets, the less loose his joints will be. So the main task of parents in this case is to prevent premature wear of the joints.
A certain diet. Dishes included in your baby's daily menu should be rich in calcium. These are dairy products, cottage cheese products, fish (preferably sea). Dishes rich in collagen are very healthy - jellied meat, aspic, jelly.
Drinking regime. As for cases of a decrease in the amount of synovial fluid inside the joint capsule, here you also need to take care of the joints, without provoking their premature wear and tear. In addition, let your child drink more, because water stimulates the production of fluid inside the joints.
A child’s joints are cracking: examination plan
Various laboratory and instrumental studies will help exclude or diagnose diseases in a child.
Laboratory diagnostics. In case of joint hypermobility, the doctor primarily focuses on the presence of complaints and accompanying diagnoses. But you will have to take tests: a general blood and urine test (this can identify acute inflammatory processes), a biochemical blood test (to determine rheumatoid factor, C-reactive protein, alkaline phosphatase, creatine kinase).
Ultrasound of joints will help identify dysplasia and determine the amount of intra-articular lubrication. Sometimes the doctor also prescribes a heart ultrasound for a small patient to identify valve pathology.
Crackling joints: alarming symptoms
Parents should be wary of cracking joints in a child under one year old if:
Only a certain joint (hip, shoulder, knee) constantly crunches;
Clicks are heard during flexion and extension movements;
Crunching in the hip joints is combined with asymmetry of the skin folds on the legs, and the hips are difficult to separate (this indicates subluxation or dislocation of the hip);
Joints crack for a long time;
With passive or active movements, the crunch is accompanied by the child's restlessness or crying;
the crunch is combined with swelling and redness of the skin in the joint area.
If you notice any of these symptoms in your child, consult a doctor immediately.
Contents [Show]
A joint is an organic connection of two or more bones. The integrity and mobility of the skeleton of an adult and a child is achieved thanks to the joints. A person’s ability to move and perform various manipulations is also determined by the presence and functioning of joints. Bone joints can be fixed (skull bones), with limited mobility (spine) and completely mobile (shoulders, elbows, pelvis, knees). Joints bother people not only in old age. Many children have problems with joint diseases from the first years of their birth. So, let's learn about the causes of various joint diseases, their types and treatment.
Causes of joint disease in children
Joint diseases in children can occur for a number of reasons. They can be the result of the natural growth and development of the child’s body, which is accompanied by rigidity and a significant decrease in the child’s mobility threshold. Also, joint diseases can be caused by sprains and deformations, fractures and dislocations, such as Osgood-Spatter disease, the course of which can be complicated by sports activities. Minor injuries to muscles, tendons and ligaments, due to the preservation of elasticity and the ability to function, can be rehabilitated by ordinary rest and rest. More severe tissue damage requires long-term recovery and the possibility of surgical treatment.
Infectious diseases, excess weight, hip dislocations, injuries, muscle imbalances, diseases of the musculoskeletal system can cause joint diseases in children: lordosis, rheumatoid arthritis, elbow and hip joints.
Lordosis in children
Lordosis is a curvature of the sagittal plane of the spine, which is convex forward. The disease can be congenital or acquired.
Congenital lordosis in children is extremely rare. The disease can be physiological and pathological. Physiological lordosis is detected in almost all children and adolescents in the cervical and lumbar spine. The disease develops in the first months of a child’s life and, due to unfavorable external factors, can take on a pathological form.
The spine in children and adults should not be and is not perfectly straight. Its physiological curves act as a shock absorber, taking on the load that a person experiences during physical activity and movement, without any discomfort. An unnatural increase in the curvature of the spinal column is a consequence of painful sensations in the back, neck or lumbar region of the child. Very often, parents do not pay attention to such complaints from children.
Pathological lordosis, in turn, is divided into primary and secondary.
Pathological primary lordosis is a consequence of inflammation and tumors of the spine, spondylolisthesis. Secondary lordosis is a consequence of trauma to the musculoskeletal system, abnormal or congenital dislocation of the hip.
Pathological lordosis is manifested by severe back pain, increased fatigue of the child, and educational lag. It is the pain syndrome in the back that sharply limits the movements of a sick child. The functioning of internal organs and metabolism is disrupted. The child sleeps poorly, becomes nervous and easily excitable. He struggles to maintain balance, tensing his muscles, which causes pain. When this form of lordosis actively develops, the child’s figure begins to change dramatically: the chest becomes flat, the shoulders move forward with the head, and the stomach begins to bulge.
When treating lordosis of all types, the diseases that provoked the curvature of the spine are initially eliminated. Primary lordosis is successfully eliminated through surgery, massage and physiotherapy, as well as therapeutic exercises.
Physical education and sports are effective preventive measures that prevent the occurrence of pathological lordosis.
Scoliosis in children
Today, about 80% of schoolchildren have scoliosis of varying severity. The disease develops intensively during skeletal growth, which is why it is called childhood. Fortunately, modern treatment methods can completely cure curvatures before the final formation of the spine. After reaching the age of twenty, it is impossible to correct the posture of a person with such a disease.
Scoliosis is a deformity, a lateral curvature of the spine, which has three types and four degrees of disease.
The following forms of curvature are distinguished:
- C-shape, representing one arc of curvature;
- S-shaped, having two arcs of curvature;
- The Z-shape is the most complex curvature, having three arcs.
Treatment methods for scoliosis and duration also depend on the degree of the disease, which is called radiological:
1st degree: curvature angle from one to ten degrees;
2nd degree: curvature angle from eleven to twenty-five degrees;
3rd degree: from twenty-six to fifty degrees;
4th degree: more than fifty degrees.
Scoliosis in children occurs due to incorrect posture when walking and sitting, when the back muscles relax and their tone is absent; sedentary lifestyle, as well as congenital asymmetry of the legs and pelvis. Both the first and second causes of scoliosis can be eliminated by the parents themselves together with the child.
Recognizing this disease at its first stage is also not difficult: ask your baby to turn his back to you and take a natural, relaxed position. Signs of spinal curvature, if any, will be noticeable.
- The left shoulder blade will appear asymmetrical in relation to the right.
- One shoulder is lower than the other.
- Leaning forward will demonstrate a noticeable curvature of the body's frame.
- When the child presses his hand to his side, there will be a considerable distance from the limb to the waist.
If you find such signs in a child, immediately go to see a doctor. A timely correct diagnosis and qualified treatment will eliminate many unwanted problems with your child’s health.
Regular exercises and special massage, physiotherapeutic procedures and special orthopedic corsets will help the child get rid of spinal curvature forever. Remember that after the age of eighteen, scoliosis is very difficult to treat, and surgery may most likely be required.
You can avoid scoliosis by using prevention: skiing and swimming, ballroom dancing; the right choice of furniture on which your child sleeps and sits, strict control over the child’s posture.
Rheumatoid arthritis in children
Rheumatoid arthritis in children and adolescents is a joint disease that is characterized by a chronic progressive course. A very common disease, and the frequency of diseases among girls is two to three times higher than the frequency of diseases among boys. The cause of the development of this disease has not been reliably established, and when diagnosing it, special attention is paid to disorders of the autoimmune process, characterized by the production of lymphocytes and autoantibodies.
Children with rheumatoid arthritis experience joint pain and stiffness, as well as morning stiffness. The lesion is invariant: the disease spreads to the wrist, knee, elbow and ankle joints. A medical examination reveals their deformation in the form of swelling, and later the formation of limited mobility of the limbs. The disease may be accompanied by enlarged lymph nodes, the formation of subcutaneous nodules that are not painful to the touch, located near the elbows. Initial and serious damage to the peripheral nervous system and internal organs: heart, lungs and kidneys, as well as increased body temperature, cannot be excluded.
If you suspect such a disease, you should immediately consult a doctor for diagnosis and prescribe further therapy.
An experienced doctor should treat rheumatoid arthritis in children. Treatment must be comprehensive and comprehensive.
Elbow joint diseases in children
A common source of elbow joint disease in young children is dislocation. The cause of subluxation of the main radioulnar joint is the careless handling of children by adults who pull the hand of a small child without feeling their strength, thereby harming his health. The peak incidence occurs at two or three years of age and extends to eight years. In girls, the left arm is more often affected by dislocations. Injury can occur even when pulling a child out of the bath with only one hand, and is accompanied by a barely audible click. An x-ray taken will show displacement of the radial head. Any movement of the child's elbow causes pain. Treatment does not involve surgery; the head of the radius can be easily returned to its place. Then it is necessary to check whether the child has repeated dislocations. After eight years, when the annular ligament becomes strong, subluxations no longer occur.
Diseases of the hip joints in children
If your child experiences pain in the knees, then the hip joint needs to be checked. Disease of the hip joint - arthritis - has another name - coxitis. Its occurrence is provoked by purulent tuberculosis infection and reactive arthritis.
Treatment of hip arthritis in a child begins with identifying the cause of the disease. Early stages of identifying a disease make it possible to cure it quickly and efficiently. For children with this diagnosis, in addition to inpatient examination and treatment, sanatorium-resort treatment is also indicated.
Hip dysplasia in a child is a congenital anomaly of all its elements and structures. If dysplasia in a newborn child is not treated, the consequences will be extremely severe: curvature of the spine and the occurrence of early osteochondrosis, disruption of the position of the pelvis, subluxation of the opposite joint and the development of a severe degenerative disease, dysplastic coxarthrosis, which portends early childhood disability.
If a child’s pathology is diagnosed in the first months of birth, then treatment is completed very successfully. If hip dysplasia is discovered after six months of age, treatment can be lengthy. Surgery cannot be ruled out.
One of the main rules for treating dysplasia in newborns is to use a functional treatment method that can completely restore the anatomical shape of the hip joint and maintain its mobility.
For parents, there is nothing more important than the health of their own children. Your attention to them, timely medical examinations and preventive measures aimed at maintaining health will help you avoid serious joint diseases in children. Take care of your children and give them more parental attention!
Especially for nashidetki.net - Diana Rudenko
Joint pain in children of any age can occur due to many different reasons. It may be the result of the child's natural growth and development and may be accompanied by rigidity and decreased mobility. Joint pain can result from sprains, strains, fractures, dislocations, or conditions such as Osgood-Schlatter disease, which are made more severe by exercise. Mildly injured (twisted or sprained) muscles, tendons and ligaments generally remain elastic and functional and usually only need rest to heal. Since in more severe injuries the tissue may be partially or completely torn, surgical treatment may be required for complete recovery.
Joint pain can also be caused by arthritis (inflammation of the cartilage, tendons and ligaments), muscle inflammation (myositis), bacterial infection of the bones (acute arthritis; osteomyelitis) and sometimes tumors (bone cancer). With proper treatment, joint pain due to most causes heals and disappears without complications (joint dislocations).
Joint- This is the movable part of the limb where two bones meet. Bones are held in place by ligaments (strong bands of tissue) and moved by muscles and tendons (the latter attach the muscle to the bone). Pain in any of these parts is considered joint pain.
Arthritis is an inflammation of one or more joints or their constituent tendons and ligaments (connective tissue). Inflammation is indicated by symptoms: swelling of the joint, limited movement, fever, pain and redness. More than 100 pathological conditions, such as infections and blood disorders, contribute to the development of arthritis.
If one joint is affected, they speak of monoarthritis, two or three joints - oligoarthritis, more than three - polyarthritis. Joint pain due to bacterial infection is not associated with physical activity: it occurs even when a person is physically at rest and noticeably intensifies with movement. In this case, there is swelling and redness of the skin around the joint, a feeling of stiffness - especially in the morning, there is a change in the shape and outline of the joint caused by inflammation of the articular tissues, disruption of the osteochondral surfaces of the joint and the accumulation of inflammatory fluid in its cavity. General symptoms such as feeling tired, fever, headache, weakness, and irritability also occur.
Causes of joint pain in children:
1. Septic inflammation of the joint (arthritis): can be caused by streptococci, staphylococci, influenza viruses and other common infections. Large joints are usually affected. The disease suddenly begins with fever, then swelling of the joint, pain when moving, and pain when touched. If the knee joint is affected, the child begins to limp.
2. Rheumatism: the disease is preceded by an acute infection of the upper respiratory tract. The classic form of rheumatism begins with fever and joint pain. Large joints are usually affected: knee, ankle, elbow, wrist. The pain is fleeting and moves from one joint to another. Redness and swelling may appear around the affected joint, but no irreversible changes occur. If the disease lasts for a long time, rheumatic nodules may appear around the joint. They look like dense, lentil-sized formations. They usually occur in places subject to pressure: elbows, wrists, forearms, knees. On the skin of a child with rheumatism, there are peculiar rashes: pale reddish, curved or ring-shaped spots, narrow stripes. As the disease progresses, severe heart damage develops.
3. Chronic arthritis lasts at least 6 weeks. The most common form of chronic arthritis in children is juvenile rheumatoid arthritis, but in addition there are about 50 rarer forms, including those associated with systemic lupus erythematosus (an inflammatory disease of the joints, skin and internal organs) and juvenile ankylosing spondylitis (inflammatory arthritis of the spine).
Although the peak incidence occurs between 2 and 5 years of age, juvenile rheumatoid arthritis can begin at any age, from the first months of life to 16 years. JRA develops in girls almost 2.5 times more often than in boys.
Although any joint can be affected, including the toes, hands, jaw, and Achilles tendons, the most commonly affected joints at the onset of the disease are the knees, ankles, and elbows. Depending on the specific form of JRA that has developed, other organs may be involved, including the eyes, skin, and heart. While untreated JRA becomes more and more damaging to the body, state-of-the-art medical care, including comprehensive, close medical supervision using medications, physical therapy, and sometimes surgery, can ensure a relatively normal life for most patients. children. However, even with the best treatment, not all symptoms can be controlled, and unexpected exacerbations of the disease should always be expected.
There are 3 subgroups of juvenile rheumatoid arthritis, which can be identified by characteristic signs and symptoms. This is a systemic form (involving the whole organism in the process); polyarthritis form (involving 5 or more joints in the process) and pauciarthritis form (involving less than five joints in the process).
– JRA was originally widely known as Still's disease, named after the doctor who first clearly described it in 1896. The term Still's disease is currently used to refer to a systemic form of JRA that affects about 20% of all children with arthritis. The systemic form of JRA, which is the most difficult to diagnose, can often begin with fever or rash and enlargement of the liver, spleen and lymph nodes. Despite the presence of pain in the muscles and heart, many months may pass before inflammation of the joint appears.
– The polyarthritis form accounts for 35% of children suffering from arthritis. This form often affects the small joints of the hands and feet, as well as the ankle, knee and hip joints. Usually there is symmetrical damage to the joints. So, if a certain joint on the left side of the body is affected, then the corresponding joint on the right side of the body is also affected.
– Approximately 45% of children suffering from JRA are affected by the pauciarthritis form. The onset of the disease is often gradual: the knee or ankle first swells, and parents only notice this when the child begins to limp. Joint pain is rare, especially in young children. Uveitis (persistent inflammation of the middle choroid, iris, and surrounding tissues with a network of tiny blood vessels in the middle of the eye) may also develop, which can threaten vision if left untreated. Children with uveitis usually need regular follow-up with an ophthalmologist (eye doctor) to monitor whether the eye has become inflamed. This inflammation is often asymptomatic and is not accompanied by redness or other obvious signs.
In many cases of JRA, after several months or years of active disease, spontaneous development of long-term remission (absence of active manifestations of the disease) is observed. In some cases, symptoms reappear from time to time, and only sometimes the child suffers from long-term continuous JRA.
Arthritis is characterized by the sequential appearance of pain, immobility, warmth, redness, swelling and, finally, a slight decrease in the functional activity of one or more joints. Restricted movement of the affected joint may be caused by muscle spasms or fluid buildup around the joint. In the case of systemic JRA, general malaise, including fever, rash, lethargy and loss of appetite, precedes joint involvement by up to 6 months. If JRA progresses uncontrollably, weakening and destruction of the joint may occur with severe limitation of freedom and ease of movement. When such destruction of the ankle and foot occurs, the child often develops a waddling, flat-footed gait. Lameness and a dragging gait occur when the knees and hips become inflamed and swollen. Joint damage may be accompanied by a variety of other symptoms. Often there is a low and constant temperature or, conversely, a high one, reaching a peak of more than 38.8 ° C once or twice a day. Pale red or pink, usually non-itchy, the rash becomes brighter during a fever. The size of the lymph nodes, liver and spleen increases. Sometimes there is a decrease in appetite and weight.
4. Serum sickness: is an allergic reaction to the administration of medicinal serums or drugs (for example, penicillin, aspirin, etc.). It usually occurs 6-12 days after the child comes into contact with the provoking factor. Manifested by joint pain (arthritis), fever, muscle pain, skin rash (urticaria), itching, swelling of the face and neck.
5. Joint injuries: as a rule, pain is observed in one joint. It swells, becomes deformed, and becomes red or bluish. Movement in the affected joint is limited and painful. Sharp pain occurs when there is mechanical stress on the joint. Young children from 1 to 4 years old often experience traumatic subluxation of the elbow joint, for example, in a fall when they are “dragged” by the arm by an adult. In this case, the annular ligament is torn at the site of its attachment to the radius bone of the forearm and is pinched between the head of the humerus and the radius. As a result, the child refuses to move his arm and keeps it motionless, slightly bent at the elbow and turned inward at the forearm around its axis.
6. Tuberculous arthritis: most often affects the hip joint. Externally, the disease first manifests itself as mild lameness and pain when walking, which radiates to the knee or mid-thigh. Over time, hip movement is limited in all directions, and swelling is noticed around the joint. The affected hip becomes flexed, pressed against the other leg, and slightly turned inward. If the spine is affected, the child complains of pain in the part of the body that is innervated from the diseased area of the spinal cord. He can hardly lift objects lying on the floor, walks very carefully, on tiptoes, and holds his torso straight. Likes to lie on his stomach.
Arthritis of the cervical spine causes torticollis, and the child is forced to support his head with his hands. If the disease process involves the thoracic spine, a hump develops.
Orthopedist-traumatologist
Rheumatologist
Phthisiatrician
The symptom chart is for educational purposes only. Do not self-medicate; For all questions regarding the definition of the disease and methods of its treatment, consult your doctor. EUROLAB is not responsible for the consequences caused by the use of information posted on the portal.
- Symptoms of arthritis in children
- Causes of arthritis in children
- Types of arthritis in children
- Treatment of arthritis in children
- A couple of tips for parents
It is sad to realize that such a terrible disease as arthritis does not bypass even the smallest inhabitants of our planet. But harsh statistics say that every thousand child under the age of 3 falls victim to this disease. The peak incidence is considered to be between one and three years of age, but this is purely individual. What are the symptoms and treatment methods for arthritis in children, you will learn from our material below.
Symptoms of arthritis in children
If the child is very small and is not yet able to clearly express his complaints, then it can be quite difficult to determine whether he has arthritis.
Parents should be attentive to their child's behavior. You should be wary of the following signs:
Unreasonable whims of the child with possible refusal to eat;
Lameness while walking or playing (the baby tries to walk less and does not allow touching the sore spot);
Complaints of pain without any objective reason (there was no fall or injury);
Swelling and redness in the joint area;
Difficulty raising an arm or leg;
Changes in the child's gait.
If at least one of the above symptoms is detected, you should immediately seek advice from a medical specialist.
The general symptoms of arthritis in children also include the following series of signs:
Increased body temperature;
The appearance of itchy spots and rashes on the skin around the sore joint;
Enlargement of regional lymph nodes located near the source of inflammation.
Causes of arthritis in children
Proper treatment of arthritis in children is possible only after establishing the true cause of its occurrence.
Causes of childhood arthritis include:
Infectious diseases;
Hereditary predisposition;
Decreased immunity;
Violation of metabolic processes in the body;
Traumatic injuries;
Diseases of the nervous system;
Exposure to low temperatures.
Diagnosing arthritis in children is often difficult. For example, a child suffered from an infectious disease, to which the parents did not attach much importance, and the complication was inflammation of the joints.
Types of arthritis in children
Among all the types of childhood arthritis, the following main forms can be distinguished:
Reactive form of arthritis. This is an aseptic inflammatory disease that mainly affects the joints of the lower extremities. The cause is a previous bacterial infection. Reactive forms of arthritis include urogenital and postenterocolitic arthritis. For example, the urogenital form occurs due to an existing infectious process in the organs of the genitourinary system;
An infectious form of arthritis. The occurrence of this form of the disease is facilitated by bacterial, viral and fungal infections. The location of pathogens is the joint cavity itself, into which they enter through the blood or lymph flow. The risk of infectious arthritis increases after joint trauma. Infectious arthritis is most common in children under three years of age;
Juvenile form of rheumatoid arthritis. The etiology of this disease is still not fully understood. It is believed that the determining factor is burdened heredity. Children under 16 years of age are at risk for developing juvenile arthritis. Juvenile arthritis primarily affects large joints, causing them to become enlarged and deformed. The danger of the disease lies in its rapid and steady progression, and in severe cases, even damage to internal organs is possible. The juvenile form of rheumatoid arthritis can occur with inflammation of only the joint apparatus, or may involve the lungs or heart in the process;
Ankylosing spondylitis. Most often, this disease debuts at an early age and manifests itself as a chronic inflammatory process in the peripheral joints and spinal column;
Rheumatic form of arthritis. It is a pathognomonic manifestation of childhood rheumatism. Children under 16 years of age are at risk for morbidity. For diseases such as chorea minor, ring erythema and rheumatism, the unifying feature is their infectious origin. Most often, the cause of their occurrence is streptococcal infection (tonsillitis, sore throat, pharyngitis).
Found an error in the text? Select it and a few more words, press Ctrl + Enter
Treatment of arthritis in children
Treatment of arthritis in children can last a long time, and the approach to it must be comprehensive. Along with drug therapy, special therapeutic massage and physiotherapy are used. If the disease is in the acute phase, outpatient treatment will be ineffective. The child must be in a hospital, where he can be given a special splint to immobilize the diseased joint.
Surgery for arthritis in childhood is indicated only in the presence of severe joint deformation, which can be corrected with prosthetics.
Drug therapy consists of two successive stages:
The use of non-steroidal anti-inflammatory drugs to relieve painful symptoms of the disease;
Taking medications that suppress the immune system, if we are talking about rheumatoid arthritis (immunosuppressants);
Carrying out detoxification therapy;
Strengthening the drainage function of the body.
The use of the first group of drugs helps relieve severe pain, reduce the inflammatory reaction and improve joint mobility.
The following drugs are used for the symptomatic treatment of arthritis in children::
Acetylsalicylic acid. It is a mandatory attribute of conservative drug therapy for arthritis. The advantages of this drug include its effectiveness, but it is strictly contraindicated in case of existing blood clotting disorders;
Diclofenac. Currently, experts have come to the conclusion that the use of diclofenac by children may cause erosive changes in the upper parts of the digestive tract. In addition, it is strictly contraindicated for children under 6 years of age;
Naproxen is another anti-inflammatory drug. It is indicated for the treatment of rheumatoid and juvenile arthritis in children. Its only drawback is the age restrictions. Naproxen is only indicated for children over 10 years of age.
Detoxification therapy is aimed at activating local and general immunity, harmonizing metabolic processes and normalizing blood circulation in the joint apparatus.
Stimulation of the drainage function is the key to complete removal of toxins from the source of the disease and stimulation of nutrition of the joint area.
The specifics of treatment of reactive arthritis in children are the following sequential actions:
Relief of severe pain;
Neutralization of the infectious focus.
Elimination of the consequences of the disease.
The non-steroidal anti-inflammatory drugs (NSAIDs) described above are used to relieve pain. If a child is experiencing excruciating pain that cannot be relieved by NSAIDs, one has to resort to intra-articular injections using hormonal anti-inflammatory drugs from the glucocorticoid group (methylprednisolone). Before prescribing corticosteroids, you must be sure that there are no pathogenic microorganisms in the intra-articular fluid.
To eliminate the infectious focus, in the practice of treating childhood arthritis, doctors widely use drugs from the macrolide group. Thanks to their gentle effects, it is possible to avoid serious side effects. The drugs of choice are clarithromycin, roxithromycin and josamycin.
If we talk about the intestinal etiology of the reactive form of arthritis, then, by and large, the fight against intestinal infection will be useless due to its absence at the time of diagnosis. The thing is that when arthritis develops, there is no longer any source of infection in the intestines. Only before potential immunosuppressive therapy should antibiotic therapy with aminoglycosides be administered.
If the disease has become chronic, there is a need for pathogenetic treatment. The main components of such therapy are immunomodulatory drugs that ensure stable functioning of the immune system. These drugs include taquitin, lycopid and polyoxidonium.
For rheumatoid arthritis no treatment will bring the expected result if immunosuppressants are not used. Only these remedies can stop the process of destruction of the child’s affected joints. Commonly used drugs include cyclosporine, mercaptopurine and leflunomide.
Treatment of juvenile arthritis carried out using anti-inflammatory drugs in combination with a special diet. Your child's daily diet should include foods rich in calcium. In order for the treatment to take place with maximum benefit, the regime of physical activity and rest should be properly organized.
Unconventional methods of treatment
Non-traditional methods of treating arthritis in children can serve as an excellent addition to conservative therapy.
One of the universal and very effective remedies is white, blue and pink clay. It has a pronounced anti-edematous and anti-inflammatory effect. The clay is suitable for external use in the treatment of arthritis in children over 3 years of age. It must be used in the form of a compress, which is applied to the sore joint, covered with cellophane and wrapped in woolen cloth.
To treat children over 6 years of age, you can use a decoction of thistle herb in the form of compresses and lotions. It is a good adjuvant in the treatment of rheumatoid arthritis. To prepare the decoction, you need to take 1 tablespoon of thistle herb and pour a glass of boiling water. You need to cook the broth for half an hour, then cool and strain. A small piece of gauze is moistened in the resulting decoction and applied to the sore joint; the compress should be covered with polyethylene and woolen cloth on top.
For older children, going to the bathhouse may be a good auxiliary treatment. Brief exposure to heat on your joints will help relieve pain. However, a bath is unacceptable during the acute period of the disease.
It is important to remember that this kind of procedure can be resorted to only after prior consultation with your doctor.
Prognosis for recovery
Unfortunately, arthritis is a disease that accompanies a person throughout his life. Provided the correct treatment is prescribed in a timely manner, the child will be able to lead a full life without remembering his illness. Of course, physical activity will have to be limited to the level of daily exercise, but professional sports for these children are strictly prohibited.
To prevent frequent relapses of arthritis from leading to disability, the child should immediately seek help from a medical specialist immediately after the first signs of the disease appear.
Joint hypermobility syndrome – this is the presence of complaints related to the musculoskeletal system in individuals with an excessive range of motion in the joints in the absence of signs of another rheumatic disease.
In English literature SGMS – benign joint hypermobility syndrome.
Historical reference : the term “joint hypermobility syndrome” belongs to English authors Kirk, Ansell And Bywaters, which in 1967 year, this term designated a condition in which there were certain complaints from the musculoskeletal system in hypermobile individuals in the absence of signs of any other rheumatic disease.
ETIOLOGY
It is believed that:- FHMS is a genetically determined disease with a dominant inheritance pattern. It is almost always possible to establish the familial nature of the observed joint hypermobility and concomitant pathology.
!!! Unlike the so-called differentiated connective tissue dysplasias (Marfan syndrome, severe Ehlers-Danlos syndrome, osteogenesis imperfecta), in which joint hypermobility is one of the manifestations of more severe systemic damage to the connective tissue, with VMS there are moderately expressed articular manifestations of connective tissue dysplasia .
On the other side, Acquired excessive joint mobility cannot be considered as VMS, which is observed in ballet dancers, athletes and musicians. Long-term repeated exercises lead to stretching of the ligaments and capsules of individual joints. In this case, local hypermobility of the joint(s) occurs.
Changes in joint flexibility are also observed in a number of pathological and physiological conditions:
acromegaly
hyperparathyroidism
pregnancy
RELEVANCE OF THE PROBLEM AND EPIDEMIOLOGY
Traditionally, the doctor's attention is drawn to identifying limited range of motion in the affected joint, rather than determining excess range of motion. Moreover, the patient himself will never report excessive flexibility, since he has coexisted with it since childhood and, moreover, is often convinced that all people have the same capabilities. However, for most patients, the first complaints occur during adolescence; symptoms can appear at any age. Therefore, the definitions of “symptomatic” or “asymptomatic” HMS are quite arbitrary and reflect only the state of an individual with HMS at a certain period of life.
Systemic connective tissue dysplasia manifests itself as an organ-specific medical problem. In all clinical medical specialties, nosological forms have been identified that represent nothing more than organ-specific manifestations of “connective tissue weakness”:
in cardiology, “connective tissue dysplasia of the heart” is known, including valve prolapse, myxomatous degeneration, additional chordae, MASS syndrome (Mitral valve, Aorta, Skin, Skeleton)
in orthopedics – non-traumatic habitual dislocations and dysplasia of the hip joints
in surgery – hernias of various localizations
in the internal medicine clinic th – nephroptosis and related problems
in gynecology – prolapse of the vaginal walls and uterine prolapse
in dermatology – cutis laxa
in vertebroneurology- dorsalgia, often combined with scoliosis and spondylolisthesis
in cosmetology - rough stretch marks after childbirth, early appearance of wrinkles, “sagging” folds of skin on the neck and torso
Prevalence of FHMS difficult to assess. The true prevalence of HMS syndrome is virtually unknown.
!!! Constitutional joint hypermobility (KHM) is detected in 7-20% of the adult population.
We can talk about the frequency of detection of GMS according to individual clinics, but at the same time, these data do not reflect the true picture, since most patients with GMS syndrome do not require hospital treatment or, due to the already mentioned insufficient knowledge of doctors about this pathology, these patients are often are registered under other diagnoses - early osteoarthritis, periarticular lesions, etc. :
In one of the large European rheumatology clinics, this diagnosis was established in 0.63% of men and 3.25% of women out of 9275 patients admitted for inpatient examination
According to domestic data, the proportion of patients with FHMS is 6.9% at an outpatient appointment with a rheumatologist
According to a survey of practicing rheumatologists in the UK, each of them sees 25–50 patients with this disease per year
According to M. Ondrasik, who examined the Slovak population aged 18-25 years (1299 people), a mild degree of hypermobility (3-4 points according to Beighton) occurred in 14.7%, severe (5-9 points) - in 12, 5%, generalized (in all joints) - in 0.7%; that is, increased joint mobility was found in almost 30% of the young people examined, the ratio of females and males was the same.
Epidemiological studies using clinical tests have established widespread hypermobility in 10% of the European population and 15-25% of the African and Asian population.
In other studies, women predominated in varying ratios to men - 6:1 and even 8:1
Among the examined children, increased joint mobility was detected in various studies in 2-7%.
As for children, the following general patterns have been established::
In children in the first weeks of life, articular hypermobility cannot be detected due to muscle hypertonicity; it occurs in almost 50% of children under 3 years of age, at 6 years of age it is detected in 5%, and at 12 years of age - in 1% (in at least three paired joints)
In young children, this syndrome occurs with equal frequency in boys and girls, and in puberty - more often in girls
The decrease in the number of people with increased joint mobility occurs quickly in childhood as the child grows and connective tissue matures; the slowdown peaks after the age of 20 years
PATHOGENESIS
The pathogenesis of VHMS is based on a hereditary feature of the structure of the main connective tissue protein - collagen, leading to greater than normal extensibility.
Biochemical and molecular studies confirmed that in hypermobility syndrome there are connective tissue disorders. Collagen analysis of skin samples from patients with hypermobility syndrome showed a violation of the normal ratios of collagen subtypes and abnormalities in the microscopic structure of connective tissue. In 1996, the British Society of Rheumatology reported the identification of mutations in fibrillin genes in several families with hypermobility syndrome.
Despite in-depth research, the pathogenesis of generalized joint laxity in hypermobility syndrome remains unclear. It seems likely that normal joint development and function require the interaction of a number of genes encoding the structure and assembly of joint-related connective tissue proteins.
Pathogenesis of complaints The joint effects of patients with hypermobility syndrome can be best understood by considering the underlying structure of the joint. The degree of joint mobility is determined by the strength and flexibility of the surrounding soft tissues, including the joint capsule, ligaments, tendons, muscles, subcutaneous tissue and skin. It has been hypothesized that excessive joint motion leads to inappropriate wear and tear of the articular surfaces and surrounding soft tissues, resulting in symptoms attributable to these tissues. Clinical observations of increased symptoms associated with excessive use of hypermobile joints provide further support for this hypothesis. Recent observations have also confirmed decreased proprioceptive sensitivity in the joints of patients with hypermobility syndrome.
Findings such as these have led to the suggestion that impaired sensory feedback contributes to excess joint injury in affected individuals.
CLINICAL MANIFESTATIONS OF VHMS
VHMS is an easily identifiable clinical sign that reflects the condition of not only the musculoskeletal system, but the entire connective tissue matrix. This approach is implemented in the international recognition of the term “hypermobility syndrome,” which currently most fully characterizes the condition of undifferentiated connective tissue dysplasia:
the name indicates generalized joint hypermobility as an important clinical sign
the absence of the word “joint” in the definition reflects the complexity of the problem, which is not limited to the musculoskeletal system
Signs of joint hypermobility (Beighton criteria)
passive flexion of the metacarpophalangeal joint of the 5th finger in both directions
passive flexion of the 1st finger towards the forearm when flexing at the wrist joint
hyperextension of the elbow joint over 10 degrees.
hyperextension of the knee joint over 10 degrees.
bend forward with fixed knee joints, while palms reach the floor.
Hypermobility is assessed in points:
A score of 1 indicates pathological hyperextension in one joint on one side.
Maximum value indicator, taking into account two-way localization, - 9 points (8 - for the first 4 points and 1 - for the 5th point).
Index from 4 to 9 points is regarded as a state of hypermobility.
Let's consider the clinical manifestations of VHMS.
JOINT MANIFESTATIONS
1.1 Arthralgia and myalgia.
The sensations may be painful, but are not accompanied by visible or palpable changes in the joints or muscles.
The most common localization is the knee, ankle, and small joints of the hands.
In children, severe pain in the hip joint has been described, responding to massage.
The severity of pain is often influenced by the emotional state, weather, and the phase of the menstrual cycle.
1.2 Acute post-traumatic articular or periarticular pathology, accompanied by:
synovitis
tenosynovitis
bursitis
1.3 Periarticular lesions - tendinitis, epicondylitis, other enthesopathies, bursitis, tunnel syndromes.
They occur in patients with FHMS more often than in the general population.
They occur in response to an unusual (unusual) load or minimal trauma.
1.4 Chronic monoarticular or polyarticular pain.
In some cases, accompanied by moderate synovitis provoked by physical activity.
This manifestation of VHMS most often leads to diagnostic errors.
1.5 Repeated dislocations and subluxations of joints.
Typical localizations - brachial, patellofemolar, metacarpophalangeal joints.
Sprained ligaments in the ankle joint.
1.6 Development of early (premature) osteoarthritis.
This may be like true polyosteoarthrosis nodosa
There may also be secondary damage to large joints (knees, hips), which occurs against the background of concomitant orthopedic anomalies - flat feet, unrecognized dysplasia of the hip joints.
1.7 Back pain (for more details, see further in the text (1), (2), (3), (4)).
Thoracalgia and lumbodynia are common in the population, especially in women over 30 years of age, so it is difficult to make an unambiguous conclusion about the connection of these pains with joint hypermobility.
Spondylolisthesis is significantly associated with GMS.
1.8 Symptomatic longitudinal, transverse or combined flatfoot and its complications:
medial tenosynovitis in the ankle area
hallux valgus and secondary arthrosis of the ankle joint - longitudinal flatfoot
posterior talar bursitis
thalalgia
"corns"
Hammer finger deformity
hallux valgus (transverse flatfoot)
(1)
The most common manifestation of spinal damage in GMS is dorsalgia. Of course, this is a symptom, but not a diagnosis. In the population (especially in older age groups) this is the most common complaint from the musculoskeletal system.
Dorsalgia in persons without HMS occurs with a frequency of 12% (among men 16–20 years old) to 35% (among women 41–50 years old). Among people with HMS, the prevalence of dorsalgia is much higher - from 35% among men 16–20 years old to 65% among women 41–50 years old. !!!
Qualitative differences in dorsalgia among hypermobile individuals consisted of a significant predominance of thoracalgia in comparison with non-hypermobile individuals, in whom lumbodynia predominated. In most cases, X-ray examination did not reveal any structural causes of dorsalgia.
Clinical manifestations of dorsalgia during HMS are nonspecific:
pain appears or intensifies with prolonged static loads - standing, sometimes sitting
decrease or disappear when lying down
decrease or disappear with adequate treatment, including taking centrally acting muscle relaxants, analgesics or non-steroidal anti-inflammatory drugs (NSAIDs), massage and gymnastics that strengthen the paravertebral muscles
It should be noted that the cause of dorsalgia in people with HMS can also be true inflammatory diseases of the spine, which occur in the population with a frequency of 0.1–0.2%. In this case, there is a different inflammatory rhythm of pain with a maximum at night and in the morning and a more distinct effect of NSAIDs.
(2) The second most common lesion of the spine in GMS is scoliosis. In the population, scoliosis occurs with a frequency of 5–7%, does not differ by gender and usually develops in childhood. With HMS, the incidence of scoliosis is 30–35%. The pain syndrome in scoliosis is nonspecific and corresponds to the above description of dorsalgia with GMS, but is more severe and persistent. Orthopedic care should be provided as early as possible. It is known that after adolescence (and in some cases even with timely intensive treatment) there is no cure.
(3) Spinal osteochondropathy (Scheerman-Mau disease) is classified in ICD-10 as juvenile osteochondrosis. The prevalence of Scheerman–Mau disease (based on radiological signs) in the population is 2–5%. In the study by Maslova E.S. the presence of this pathology was shown in 11% of patients with HMS (almost always combined with clinical kyphoscoliosis) and in 2% of non-hypermobile individuals in the control group. Clinical manifestations of Scheerman–Mau disease do not differ in specificity and correspond to the above-described picture of dorsalgia with GMS, differing only in persistence, a tendency towards lifelong persistence of spinal deformity and the development of radiological signs of secondary osteochondrosis at a young age.
(4) Spondylolisthesis (persistent displacement of the vertebral bodies in the horizontal plane) is most logically united by the common pathogenesis with GMS. One of the causes of spondylolisthesis is increased extensibility of the powerful ligamentous apparatus of the spine. Another factor that stabilizes the position of the vertebrae is the condition of the arcuate joints. Apparently, the latter is associated with the relative rarity of detection - 0.5-1% (compared to other types of spinal pathology) - spondylolisthesis in HMS. Despite its rarity, this spinal lesion in GMS is the most specific, which is reflected in the inclusion of spondylolisthesis as a separate sign in the criteria for the diagnosis of GMS. Spondylolisthesis in HS may be accompanied by signs of persistent mechanical radiculopathy and require surgical stabilization of the affected vertebral segment.
2. EXTRA-ARTICULAR MANIFESTATIONS
These signs are natural, since the main structural protein collagen, which is primarily involved in the described pathology, is also present in other supporting tissues - fascia, dermis, vascular wall.
2.1 Excessive extensibility of the skin, its fragility and vulnerability. Striae not associated with pregnancy.
2.2 Varicose veins that begin in young years.
2.3 Mitral valve prolapse.
2.4 Hernias of various localizations (umbilical, inguinal, white line of the abdomen, postoperative).
2.5 Prolapse of internal organs - stomach, kidneys, uterus, rectum.
2.6 Respiratory system: tracheobronchomegaly, spontaneous pneumothorax, emphysema, recurrent bronchopneumonia, obstructive bronchitis.
2.7 Genitourinary system: anomalies, polycystic disease, diverticulosis of the bladder.
2.8 Teeth: abnormal location, irregular formation, enamel hypoplasia, gum resorption, tooth loss, multiple caries, etc.
2.9 Neurovegetative manifestations and mental abnormalities are observed.
Considering the widespread prevalence of constitutional HMS in the population, especially among young people, it would be erroneous to explain all joint problems in this category of people only by hypermobility. The presence of HMS does not at all exclude the possibility of them developing any other rheumatic disease, to which they are susceptible with the same probability as persons with a normal range of motion in the joints.
!!! The diagnosis of HMS syndrome becomes justified in cases where:
other rheumatic diseases are excluded
the existing symptoms correspond to the clinical signs of the syndrome
logically complemented by identifying excessive joint mobility and/or other markers of generalized connective tissue involvement
CRITERIA FOR HYPERMOBILITY SYNDROME
Large criteria
Beighton score 4 out of 9 or higher (current or past)
arthralgia lasting more than 3 months involving 4 or more joints
Small criteria
Beighton score 1, 2, or 3 out of 9 (0, 1, 2, or 3 if age 50+)
arthralgia (1-3 joints) or back pain, spondylosis, spondylolysis, spondylolisthesis
dislocation (dislocation/subluxation) of more than one joint or one joint more than once.
three or more soft tissue lesions (eg, epicondylitis, tenosynovitis, bursitis)
marfanoid habitus (tall, thin, arm span greater than height, upper to lower segment ratio 0.89, arachnodactyly)
skin: stretch marks, hyperextensibility, thin skin or abnormal scarring
Ocular manifestations: drooping eyelids, myopia or antimongoloid oblique incision of the eyes
varicose veins, hernia or uterine prolapse/rectal prolapse
Mitral valve prolapse (on echocardiography)
!!! Hypermobility syndrome is diagnosed if there are two large or one large and two small criteria or 4 small criteria.
!!! Two small criteria are sufficient when there is clearly an ill first-degree relative.
!!! Hypermobility syndrome is ruled out based on the presence of Marfan syndrome or Ehlers-Danlos syndrome as defined by Berlin nosology.
T.Milkowska-Dmitrova and A.Karakashov
offer the following criteria for diagnosing congenital connective tissue deficiency:
main: flat feet, varicose veins, gothic palate, stretched joints, eye changes and osteoligamentous symptoms - kyphosis, scoliosis, hyperlordosis
minor: abnormalities of the auricles, joint pain, pterygium, dental anomalies, hernias, hypertelorism, etc.
Along with the clinical assessment of connective tissue dysplasia, they play an important role in the diagnosis of the disease. BIOCHEMICAL RESEARCH METHODS
. They allow:
assess the state of connective tissue metabolism
clarify the diagnosis
predict the course of the disease
The most informative is:
level determination hydroxyproline and glycosaminoglycans in daily urine
definition lysine, proline, hydroxyproline in blood serum
Genetic defects in collagen synthesis lead to a decrease in its cross-links and an increase in the number of easily soluble fractions. That is why in patients with congenital connective tissue dysplasia there is a significant increase in hydroxyproline in daily urine, the degree of which correlates with the severity of the pathological process. The catabolism of the intercellular substance is judged by the amount of excretion of glycosaminoglycans.
Hereditary connective tissue diseases are characterized by changes in the ratio of different types of collagens and disruption of the structure of collagen fiber.
Collagen typing carried out by the method of indirect immunofluorescence according to Sternberg L.A. using polyclonal antibodies to fibronectin and collagen.
Modern and promising ismolecular genetic diagnostics (DNA diagnostics) of connective tissue dysplasia, which involves the use of molecular methods for identifying gene mutations.
Molecular analysis of the fibrillin1 (FBN1) gene if Marfan syndrome is suspected, it can be performed on genomic DNA extracted from blood leukocytes. In cases of diagnosis of Ehlers-Danlos syndrome or osteogenesis imperfecta, a skin biopsy is performed followed by biochemical analysis of collagen types I, III and V.
Depending on the clinical and biochemical assessment, further molecular analysis is performed on DNA extracted from cultured fibroblasts .
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of hypermobility includes a wide variety of genetic and acquired disorders, and it is important to consider each of these possibilities when assessing a child who presents with generalized joint laxity.
Differentiating hypermobility syndrome from other connective tissue disorders is a particularly common diagnostic dilemma. Further, asymptomatic hypermobility can often be identified on routine physical examination, suggesting the possibility of an undiagnosed connective tissue disorder. For this reason, it is critical for the clinician to recognize the hallmarks of inherited connective tissue disorders in children with hypermobility.
Ehlers-Danlos syndrome
Ehlers-Danlos syndrome (EDS) refers to a group of connective tissue disorders that share characteristics with joint hypermobility and skin abnormalities. Skin manifestations may range from softness, thinning, or hyperelasticity to extreme susceptibility to tearing and bruising and abnormal scar formation. There are 10 subtypes of EDS, which differ in terms of severity of joint and skin manifestations, involvement of other tissues and mode of inheritance. Specific molecular defects in collagen or enzymes involved in the formation of connective tissue have been identified in some subtypes of EDS.
Most cases of EDS are types I, II and III. The most severe joint laxity is observed in EDS type I; Patients experience significant hypermobility, often accompanied by pain, effusion, and dislocation. Children with this condition may have congenital hip dislocations, club feet, or a delay in walking due to joint symptoms and leg instability. Associated skin manifestations include soft, stretchable skin with a velvety texture, a tendency to bruise, and the formation of thin, cigarette paper-like scars when injured. EDS type II is similar to EDS type I, but less severe. Both disorders are caused by defects in type V collagen and are inherited in an autosomal dominant manner.
Autosomal recessive inheritance of EDS type II caused by other collagen defects has been reported, but is rare. EDS type III is similar to type I in terms of joint involvement, but skin abnormalities are usually limited to an abnormally soft and velvety skin texture.
For this reason, EDS type III is often confused with hypermobility syndrome, which is generally considered to have few or no skin lesions. From a practical point of view, however, the clinical differences are minimal and both disorders should be managed in a similar manner. EDS type III is transmitted in an autosomal dominant manner, and the exact molecular defect is unknown.
Of all the rarer subtypes of EDS, EDS type IV is the most important to recognize. Although joint and skin abnormalities are usually mild, these patients are at significantly increased risk of potentially fatal spontaneous rupture of arteries and hollow organs such as the colon. Women with EDS type IV may experience uterine rupture during pregnancy. This autosomal dominant disorder is caused by defective type III collagen. It should be noted that a revised EDS clinical classification system has been proposed.
Marfan syndrome
Marfan syndrome is an autosomal dominant disorder characterized by a long, thin body (marfanoid habitus), long limbs, elongated fingers (arachnodactyly), ocular abnormalities (myopia, lens dislocation), and generalized joint laxity. It is caused by mutations in the fibrillin-1 gene on chromosome 15. Fibrillin is an essential glycoprotein component of elastic connective tissue. Recognition of this disorder is very important because patients are predisposed to life-threatening aortic aneurysms and dissection, as well as aortic valve regurgitation and mitral valve prolapse.
Because of the serious nature of Marfan syndrome, any child suspected of having the condition should undergo genetic, cardiac, and ophthalmologic testing. As part of this diet, plasma amino acid analysis should be performed to rule out homocystinuria, a metabolic disorder in which there is excessive accumulation of homocystine. In most cases, this occurs as a result of insufficient activity of the enzyme cystathionine synthetase. Clinically, homocystinuria is very similar to Marfan syndrome in terms of body habitus, lens dislocation, and generalized joint laxity. However, patients with homocystinuria may have mental retardation and are at significant risk for arterial thrombosis.
Osteogenesis imperfecta
Osteogenesis imperfecta, an autosomal dominant disorder of collagen, is characterized by thin blue sclera, excessive joint mobility, and bone fragility, often leading to multiple fractures and bone deformities. The disorder is highly variable, often resulting from sporadic mutation, and includes both lethal and non-lethal forms. Lethal forms imply severe bone fragility, which is incompatible with life. Non-lethal variants may have milder clinical manifestations, with complications associated with fractures, joint instability, short stature and progressive spinal deformity. The latter problem can lead to cardiorespiratory failure, and effective surgical correction is difficult due to the fragility of the bone. In adulthood, progressive otosclerosis often leads to deafness.
Stickler syndrome
Stickler syndrome is an autosomal dominant disorder that is characterized by hypermobility, characteristic facial features (zygomatic hypoplasia with depressed nasal bridge and epicanthus), Robin sequence (micrognathia, glossoptosis, and cleft palate), early arthritis, severe myopia, and sensorineural hearing loss.
Affected infants often have respiratory problems associated with the Robin sequence, and older children may develop arthritis before adolescence. Severe myopia and an increased risk of retinal detachment necessitate frequent ophthalmic evaluation.
Williams syndrome
Williams syndrome is another autosomal dominant disorder characterized by hypermobility. However, joint laxity is observed mainly in childhood; in older patients, joint contractures may develop. These patients also have short stature, a distinctive facial structure, a rough voice, developmental delay (an outgoing cocktail party personality), and episodic hypercalcemia. Patients may have a congenital cardiovascular disorder, most commonly supvalvular aortic stenosis, and are predisposed to developing other vascular stenoses. It was recently discovered that this syndrome results from deletions in the long arm of chromosome 7, which always includes the elastin gene region. Definitive diagnosis is possible through molecular testing.
TREATMENT
Treatment of a patient with HMS syndrome depends on the specific situation. The variety of manifestations of the syndrome also requires a differentiated approach to each individual patient. The important point is explaining in an accessible form the reasons for his joint problems (“weak ligaments”) and convincing the patient that he does not have a serious illness that threatens inevitable disability. For moderate arthralgia this is sufficient. Will be useful recommendations to eliminate stress that causes pain and discomfort in the joints. Decisive in the treatment of severe pain are non-drug methods, and first of all, optimizing lifestyle. This involves matching the loads and the threshold of their tolerance for a given patient. It is necessary to minimize the possibility of injury, which includes vocational guidance and the exclusion of team sports.
For persistent pain in one or more joints use elastic orthoses (knee pads, etc.). Timely correction of detected flat feet is very important. Wherein required from the doctor basic podological knowledge - the shape and rigidity of the insoles is determined individually, the success of treatment largely depends on this. It is often possible to cope with persistent arthralgias of the knee joints using this only method.
To ensure joint stability Not only the ligaments play a significant role, but also the muscles surrounding the joint. If it is impossible to influence the condition of the ligamentous apparatus through exercises, then strengthening and increasing muscle strength is a real task. Gymnastics with GMS syndrome has a peculiarity - it includes so-called “isometric” exercises, during which significant muscle tension occurs, but the range of movements in the joints is minimal. Depending on the location of the pain syndrome, it is recommended to strengthen the muscles of the thighs (knee joints), shoulder girdle, back, etc. Swimming is useful.
Drug therapy applicable as a symptomatic treatment for arthralgia. Since the pain associated with GMS syndrome is mainly non-inflammatory in nature, it is often possible to see a complete lack of effect from the use of non-steroidal anti-inflammatory drugs.
In this case, greater results can be achieved by taking analgesics (paracetamol, tramadol). Intra-articular injection of corticosteroids in the absence of signs of synovitis is absolutely ineffective.
For periarticular lesions(tendonitis, enthesopathies, bursitis, tunnel syndromes) treatment tactics are practically no different from those in ordinary patients. In moderate cases this is an ointment with non-steroidal anti-inflammatory drugs in the form of applications or compresses; in more stubborn- local administration of small doses of glucocorticosteroids that do not have a local degenerative effect (suspension of methylprednisolone crystals, betamethasone). It should be noted that the effectiveness of local corticosteroid therapy largely depends on the correctness of the topical diagnosis and the technique of performing the procedure itself.
In terms of correction of dorsalgia with HMS, a very important role belongs to central muscle relaxants.
Their use allows:
on the one hand, to achieve a more pronounced therapeutic effect
on the other hand, reduce the daily dose of NSAIDs and, accordingly, reduce the risk of developing NSAID-associated adverse events
Among centrally acting muscle relaxants, it has proven itself well tolperisone (Mydocalm), which has been successfully used for many years in many diseases accompanied by increased muscle tone. Daily dosage Mydocalm in most cases is 450 mg (divided into 3 doses), duration of treatment Mydocalma depends on the patient's condition. The effect of including Mydocalm in the drug complex is not only reduction of pain syndrome, but also increasing range of motion. The latter circumstance affects another important aspect in the prognosis of the course and correction of dorsalgia, namely opportunity for the patient to complete a physical rehabilitation program. It is well known that the more carefully a patient follows the recommendations for physical rehabilitation, the better his functional prognosis. Respectively, reduction of reflex muscle spasm allows you to achieve a greater range of movements in the spine when performing physical exercises.
Main role in the correction of scoliosis belongs physical methods of influence. However, it is advisable to supplement rehabilitation programs with the use of muscle relaxants, and, if necessary, also analgesics or NSAIDs. This can significantly improve both the quality of life and the patient's ability to participate in a rehabilitation program.
Principles of therapy for Scheuermann–Mau disease consist of as much as possible early onset, using methods that correct posture, optimizing lifestyle (sleeping on a hard bed, lifelong therapeutic exercises, including sports that strengthen the dorsal muscles– tennis, swimming), back muscle massage. As with symptomatic scoliosis, course use of muscle relaxants is periodically indicated, and, if necessary, NSAIDs as symptomatic therapy.
The general principles of therapy for a patient with HS are the following:
complexity of the approach, i.e. a look at all the patient’s health problems (not only with the musculoskeletal system) through the prism of a possible generalized “failure” of connective tissue. Often this approach allows us to combine pathological manifestations from various body systems with one cause and one diagnosis
special attention is paid to non-drug methods of treatment and rehabilitation
explaining to the patient the need for long-term, sometimes lifelong, compliance with recommendations aimed at correcting and preventing further progression of spinal deformity, increasing and maintaining the strength of the paravertebral muscles
symptomatic treatment (analgesics or NSAIDs) should be used with caution (risk of side effects)
For pathogenetically oriented drug therapy of pain syndrome in HS, central muscle relaxants (Mydocalm) are used.
FORECAST
Because joints tend to become stiff with age, the natural history of hypermobility syndrome is usually one of improvement with progressive improvement in the degree of joint laxity and associated musculoskeletal symptoms. For many affected children, symptoms disappear during adolescence or adulthood, and women may experience a decrease in symptoms after menopause.
Although hypermobility syndrome is relatively benign condition, in patients with this syndrome an increased incidence of some potentially significant symptoms has been reported. In studies involving football players and ballet dancers with hypermobility, increased incidence of ligament ruptures, joint dislocations and other orthopedic disorders. Individuals with this syndrome may be prone to fractures, and as a result of hypermobility of the spine scoliosis may occur. Some clinicians have observed increased incidence of hernia, and uterine prolapse and rectal prolapse in adults with hypermobility syndrome.
Finally, it has been suggested that children with hypermobility syndrome have an increased risk of developing premature degenerative osteoarthritis as adults. A specific progression pattern has been described by some clinicians, including the onset of arthritis in the 4th to 5th decade of life, which is eventually followed by chondrocalcinosis of the affected joints.
However, much of the evidence for this association has been anecdotal, and it remains the subject of considerable debate. It is generally agreed that only long-term prospective studies of patients with hypermobility syndrome will provide insight into the natural history and prognosis of this common and often unrecognized disorder.
NB!!! HMS is a common rheumatic syndrome that is not prognostically dangerous, but causes serious diagnostic problems in practice. A patient with suspected HMS syndrome requires the physician to pay attention to subtle details during history taking and examination; knowledge and experience are required in the ability to determine to what extent the nature of the complaints corresponds to the unusual joint mobility being detected. Treatment of GMS syndrome also has its own specifics and differs from traditional therapy for other patients with joint diseases.
Alarming symptoms
Clicking joints should not always alarm parents. However, there are signs that cannot be ignored.
Alarming symptoms are:
- One joint cracks systematically.
- The violation continues for a long time.
- The sound is heard when flexing and extending parts of the body.
- Asymmetry of skin folds on the legs and difficult separation of the limbs are revealed.
- The child is worried, capricious, and cries when crunching.
- There is swelling and redness in the joint area.
If these manifestations are detected, you should consult a doctor.
Causes of crunching in joints
In an infant
Young mothers worry about the health of their newborn children: at this age, the child is often exposed to pathologies. Crunching in the baby's joints also makes parents wary.
The causes of the phenomenon are the following factors:
- Age. In this case, the joints of a child under one year old crack due to growth. The symptom is due to the fact that the baby’s muscle and connective tissues are at the stage of development. It disappears on its own when the baby begins to walk.
- Heredity. Insufficient formation of joints, bones and ligaments is often passed on to children from parents.
- Inflammation of the joint. During the pathological process, the sound is often heard and is accompanied by anxiety, crying, swelling, and redness of the affected area. The disorder is called arthritis. The disease most often affects the knee and requires urgent treatment measures to avoid dangerous complications.
- Hip dysplasia. The pathology is characterized by asymmetry of the inguinal folds, difficulties in abducting the limbs, and differences in the length of the legs. The disease also requires immediate medical attention. The younger the child, the easier it is to get rid of dysplasia.
In children from 3 to 8 years old
If a child of this age experiences crunching in the joints, you should be wary: the clicks are often pathological.
- Height. Joints crack due to intense growth of the body. This is considered the norm. The musculoskeletal system develops quickly, and synovial fluid does not have time to form in the required quantity. This is where the clicks come from.
- Deficiency of vitamins and microelements. During the period of growth, the child requires nutrients. An important component for joints is calcium, the lack of which leads to crunching.
- Fluid deficiency. If there is not enough water in the body, the level of intra-articular fluid drops. This leads to loss of elasticity of the joint elements, which causes crunching.
- Physical exercise. When a child is introduced to sports, the body does not immediately get used to it, so clicks appear.
- Damage. Children are often exposed to injuries that cause pathological manifestations, including crunching.
- Diseases. Joints can crack due to various ailments affecting joints and bones. But in such cases, the sound is accompanied by other symptoms: pain, swelling, redness, fever, limited movement.
Why do teenagers crack their joints?
- Hormonal imbalance. Teenagers experience hormonal surges and changes occur in their bodies. The process also affects the musculoskeletal system, causing clicking sounds.
- Hypermobility of joints. If a child has flexible joints from birth and weak ligaments, this will accompany him throughout his life.
- Physical exercise. Crunching in joints in teenagers can occur due to improper distribution of load when playing sports.
- Excess body weight. With a large weight, the connecting structures are heavily loaded, which causes them to crunch.
- Flat feet. The legs of children who have not cured this pathology are subject to increased pressure. The response to this is a crunch in the joints.
- Injuries. Activity often leads to dislocations, fractures and other injuries that cause clicking.
- Diseases. An inflammatory process in the joint area can cause a crunch. It is accompanied by pain and limited movement.
Diagnostic measures
If you notice a crunching sound in a child, you should consult a doctor. He will study the symptoms, medical history and prescribe a diagnosis.
In addition to laboratory diagnostics, you will need to do an ultrasound examination. It helps to identify dysplasia and determine the amount of synovial fluid. Sometimes young patients are prescribed a heart ultrasound to ensure normal valve function.
Treatment
Medicines
For cracking joints, the doctor prescribes medications in any form - injections, tablets and ointments. Doctors usually recommend taking anti-inflammatory non-steroidal medications to help restore cartilage.
If necessary, patients are required to take medications that stimulate the immune system and antibacterial agents. It is important to take vitamin and mineral complexes when crunching.
Traditional methods
Alternative medicine offers effective recipes to help restore joints:
- Sunflower root decoction. Excellent for removing salts from the body. Brew 100 g of the plant with a liter of water, boil for 10 minutes. Then let it cool, strain and take it every day as thirst appears. The course of therapy is no more than 3 months.
- Spruce infusion. Pour 5 spruce cones into a liter of boiling water, leave for 12 hours and take 250 ml daily.
- Laurel drink. Brew 20 leaves with 500 ml of hot water, leave in a thermos for 3 hours. You need to drink the product for 3 days, then pause for a week. The entire volume received must be taken within 12 hours.
Diet food
For normal functioning of joints, the presence of sufficient nutrients in the body is required. Therefore, patients are prescribed a diet. Pasta, bread and buns made from white flour, and cookies are removed from the diet.
Useful foods for cracking joints are:
- Milk, cottage cheese, cheese, herbs, vegetables, raisins - they contain calcium.
- Fish, liver, peaches. Rich in phosphorus.
- Seafood, fish oil. They contain vitamin D.
- Eggs, rose hips, apples are a source of manganese.
Prevention
To avoid joint problems in children, prevention is necessary. It consists of maintaining an active lifestyle, but without overloading the musculoskeletal system. Sports should be moderate: exercises should be done carefully to avoid injury.
You should also follow nutritional rules. The menu is designed so that the body is fully provided with useful substances. Carefully monitor the health of your children and at the first sign of a problem, contact a specialist.
Strengthening weak joints in a child
If a child has weak joints, then possible reasons are the toxic effect of environmental factors on the developing child’s body (lack of calcium in water and soil, imbalance of microelements in food).
If the joint ceases to function normally, then this indicates either overload (during sports training, for example), or a lack of chondroitin and glucosamine in the joint, as the main components. The first and second (load and disadvantage) are interrelated.
For childhood arthritis, it is recommended to reduce the load on the joints and use drugs that eliminate pain, reduce muscle contraction, and improve the nutrition of cartilage. Plus physiotherapy (ultrasound, Bernard currents), spa treatment (mud, hydrogen sulfide and radon sources), exercise therapy, massage.
It's good for your joints to do exercises with low weights and high repetitions. This will increase the production of growth hormone and, as a result, heal the joints. Pressure and stretch resistance exercises are needed.
Fish and foods with calcium are very useful. Fish oil is very good for joints. Take a teaspoon 3 times a day.
If a small child's joints are cracking
Children's joints are very fragile. Even a slight crunch or clicking noise made by a child's joints can greatly frighten parents.
Some children actually hear cracking sounds in their joints during certain movements. The reason is the immaturity of the ligamentous-muscular system. The connective tissue of a child’s joints is not as dense as in adults and is more elastic. The muscular system is much less developed, which is why the joints crack. As the joints grow (when the child gets older), the crunching goes away, so there’s nothing wrong with that.
But if only one joint cracks, and the crunch does not go away with age, this may be a harbinger of joint pathology or the beginning of any diseases of the musculoskeletal system. Sometimes cracking joints is an anatomical feature; it can be corrected with proper nutrition.
Calcium, phosphorus, vitamin D and manganese are very necessary. You need to drink enough fluids throughout the day, because... water stimulates the production of intra-articular fluid.
General recommendations for joints: less monosaccharides (cookies, pasta, baked goods made from white flour), more polysaccharides (potatoes and other vegetables, fruits, oat and whole grain bread). Ears, pork tails (jellied meat), cottage cheese, milk, hard cheeses, and chicken eggs are useful.
Ears and tails are a source of naturally occurring collagen. Collagen is a constituent protein of connective tissue. Connective tissue - muscles, ligaments, bones, cartilage, joints, blood vessels, parenchyma of internal organs, skin, nails, hair, dentin of teeth and joints.
Collagen hydrolyzate can be obtained by cooking - this is what we call jellied meat.
Manganese is a carrier of oxygen from the blood to the cells of the body; it is especially important for the nutrition of cartilage and intervertebral discs, because they do not have direct blood circulation. If there is a lack of manganese, the ossification processes in the skeleton are disrupted - the joints are deformed, the tubular bones become thicker and shorter.
Products that are good for joints
For calcium, it is best to: boil the eggs, peel the film from the shell, and crush them. Take a teaspoon up to three times a day with a drink. The taste is not very pleasant, but it helps a lot with calcium deficiency.
Magnesium is found in dates, prunes, raisins, dried apricots, beans, soybeans, buckwheat honey, oatmeal and buckwheat, nuts, bran, whole grain bread, dark chocolate, cocoa.
Selenium is interconnected with vitamin E - consumption of one requires proportional consumption of the other.
Vitamin D prevents the leaching of calcium from bones: it is found in fish liver, butter, cottage cheese, cheese, dairy products and egg yolk.
Joints need vitamins B, C, E, A, K, as well as microelements. Vitamin F is a complex of polyunsaturated fatty acids that has an anti-inflammatory effect. Salads made from raw vegetables, seasoned with olive or other vegetable oil, are very good for joint health.
Collagen is a complex protein that forms the basis of all human connective tissue, which is approximately 25-35% of the total protein mass in the body.
A lot of polyunsaturated fatty acids are found in fatty sea fish: regular herring works well here; it is better to buy it frozen or lightly salted. Salted herring can be soaked in milk, and after that it can be given even to children from 2 years old.
Fruits and vegetables should be cooked as little as possible, and peeled and cut immediately before consumption to preserve vitamin C.
Collagen synthesis in the body is a complex biochemical process that involves a large number of vitamins and minerals. With age, or as a result of diseases or poor nutrition, the body’s process of synthesis of its own collagen slows down, which begins to negatively affect the condition of connective tissue - it ceases to be replenished and is destroyed. In this case, the use of collagen hydrolyzate can compensate for the lack of collagen and stimulate the body to produce its own protein.
Hyaluronic acid and joints
Hyaluronic acid is one of the main components of the extracellular matrix and is found in many biological fluids (saliva, synovial fluid, etc.).
In the joint cavity there is a special synovial fluid that has a unique biological composition and properties. Its composition is similar to blood plasma, but it contains less proteins and contains hyaluronic acid, which is necessary to ensure that the fluid is viscous and the joints are constantly lubricated.
Hyaluronic acid is the main component of synovial fluid, responsible for its viscosity. Along with lubricin, hyaluronic acid is the main component of biological lubricant - an important component of articular cartilage.
The joints are covered with synovial membranes, which contain synovial fluid; and as soon as its composition deteriorates, the membranes cease to protect the joints from friction. The synthesis of hyaluronic acid in cells due to poor nutrition and negative influences slows down and even stops; In this case, the synovial fluid ceases to perform its function, and the tissues of the joints begin to quickly deteriorate. Then even children and young children develop arthrosis and arthritis.
Hyaluronic acid is part of many tissues (skin, cartilage, vitreous), and this is what determines its use in the treatment of diseases associated with these tissues (cataracts, osteoarthritis): synovial fluid endoprostheses; surgical environment for ophthalmic operations; preparations for mild tissue augmentation and wrinkle filling (including in the form of intradermal injections) in cosmetic surgery.
To ensure that the amount of hyaluronic acid in the cartilage and connective tissues, as well as in the interarticular fluid, does not decrease, it is necessary to consume foods containing mucopolysaccharides - these substances are vital for joints. An important property of these products is their gelling ability.
These are seaweed, mussels, shrimp and other seafood, as well as ligaments, bones and cartilage of fish, birds and animals - it is from these products that aspic, jellies, and jellied meats are prepared. Often these useful parts are considered waste; chicken feet, fish heads, beef and pork bones are thrown away.
Try not to throw away such waste, but cook, for example, fish soup from a fish head - the fish soup will turn out to be very rich, tasty and healthy. The fish can be any, river or sea: catfish, perch, pike, salmon, halibut, salmon fish.
Wash the heads (1-2 pieces) thoroughly, remove the gills, cut into several parts, put in a pan with cold water, cook over low heat for about an hour. It is good to cook with black pepper (6-7 peas) and bay leaf; You can also add fins and a tail.
Next, add 2 chopped onions, carrots, bell pepper and tomato, dry seaweed (2 tsp), add sea salt to taste, cook for another 5-7 minutes. Place a slice of lemon on each plate of the finished fish soup and pour in a little lemon juice. Sprinkle with fresh herbs. Excellent fish soup for joints!
Multiple micro-concussions of the joints during running cause microtrauma to the articular surfaces, which is why professional runners always have problems with their joints. Therefore, track and field athletes spend a lot of time developing their running technique, when they try to minimize these harmful effects on the joint. And you need special shoes.
But walking is very beneficial for joints. Both sports and ordinary. So walk more.
Pharmacy products for joints
Pharmacies sell various products to strengthen joints. There are many medications whose purpose is to strengthen joints and maintain the elasticity of articular joints. Such preparations contain glucosamine and collagen, because it is these substances that restore the elasticity of the cartilage structure and form the basis of connective tissue.
Chondroprotectors (Chondroitin, Glucosamine). Preserve and restore the elasticity and flexibility of cartilage;
have an anti-inflammatory effect; improve the moisture saturation of cartilage tissue;
contribute to the proper construction of new cartilage tissue;
restore joint mobility; reduce pain.
Geladrink Forte - collagen, chondroitin, glucosamine, three in one, Czech drug.
If there is an excessive intake of hyaluronic acid in the form of medical drugs or during cosmetic procedures, the skin after a certain period of time ceases to produce it on its own.
Medicinal substances that contain hyaluronic acid are divided into two types:
Hyaluronic acid preparations of animal origin are produced by distillation of animal tissue.
Medical products in which hyaluronic acid is produced by special microorganisms.
If the joints pop out
If the joints pop out, it is called a habitual dislocation. This phenomenon is also called chronic dislocation. It is expressed primarily in the weakness of the ligaments. May be as a result of a dislocation. To prevent this from happening, you need to train your muscles. Slowly, with moderate loads. Make sure that the joint does not pop out during training. But before you start training, go to the doctor. You may have torn ligaments as a result of a sprain.
First you need to reduce inflammation. Use anti-inflammatory drugs such as ketorol or voltaren. Well, limit the movement of the sore joint. And of course, massage, physiotherapy, and moderate physical activity are required.
If the pain is severe, you can apply ice to the joint.
Muscles need to be strengthened. Then there will be significantly fewer dislocations and the joints will be trained. Trained muscles are themselves a protection against popping joints.
The total duration of treatment for such dislocations is about six weeks.
But you shouldn’t give up physical activity in the future. This will only be beneficial. Exercise is life and therefore you should not stop training, even if the course of treatment is already over. Think for yourself. After all, if you quit, sooner or later the pain will return. Such is the nature of man and his organs. Where there is no load, stagnation and degradation develop. It is for these reasons that we do not recommend that you quit gymnastics.
Exercises to strengthen ligaments and tendons
This video shows techniques for strengthening ligaments and tendons. Using the example of the shoulder and elbow joints. You can train the hip and knee joints in a similar way.
What is joint hypermobility syndrome in children and adults?
Joints are designed to provide flexibility and mobility to the human body, but sometimes these properties become excessive. And then doctors talk about hypermobility syndrome or joint hypermobility.
Definition of hypermobility
Any joint can provide movement only to a certain extent. This happens due to the ligaments that surround it and act as a limiter.
In the case when the ligamentous apparatus does not cope with its task, the range of movements in the joint increases significantly.
For example, in this condition, the knee or elbow joints will be able not only to bend, but also to hyperextend in the other direction, which is impossible during normal operation of the ligaments.
Reasons for the development of joint hypermobility
There are various theories about the development of this condition. Most doctors and scientists believe that excessive joint mobility is associated with collagen stretchability. This substance is part of ligaments, the intercellular substance of cartilage, and is ubiquitous in the human body.
When collagen fibers stretch more than usual, movement in the joints becomes freer. This condition is also called weak ligaments.
Prevalence
Joint hypermobility syndrome is quite common among the population, its frequency can reach 15%. It is not always recorded by doctors due to minor complaints. And patients rarely focus on this, believing that they simply have weak ligaments.
Joint hypermobility is common in children. It is associated with metabolic disorders, insufficient intake of vitamins from food, and rapid growth.
At a young age, the syndrome is more often observed in girls. Elderly people rarely get sick.
Types of joint hypermobility
Joint hypermobility syndrome is in most cases a congenital pathology. However, it cannot be classified as an independent disease. Hypermobility of the joints is only a consequence of a disease of the connective tissue that makes up the joints and ligaments.
Often, even with the most thorough examination, connective tissue diseases cannot be identified. Then doctors talk only about a violation of its development. The joint manifestations will be the same, but the prognosis for the patient is more favorable and there are fewer complications.
There is also artificial excessive mobility of joints. It is found in sports - gymnastics, acrobatics. For musicians and dancers, choreographers, hypermobile joints are a great advantage. In this case, hypermobility is developed specifically - through persistent training, stretching of muscles and ligaments. Elastic ligaments provide the body with the necessary flexibility.
But even with the longest training, it is difficult for the average person to achieve great success.
This is usually achieved by those who initially have a predisposition to hypermobility syndrome. Therefore, artificial joint hypermobility can sometimes be considered as a pathological option along with congenital hypermobility.
Diseases in which hypermobility occurs
Joint hypermobility can be one of the manifestations of other pathologies. Today, medicine knows several such diseases:
- The most common disease in which excessive joint mobility is pronounced is Marfan syndrome. Until recently, all cases of “weak ligaments” were associated with it. People with Marfan syndrome are tall, thin, with long arms and very mobile, extremely flexible joints. Sometimes their joints resemble rubber ones in terms of flexibility, especially with regard to the fingers.
- Later, attention was paid to another disease - Ehlers-Danlos syndrome. With it, the range of joint movements is also extremely wide. It also adds to the excess elasticity of the skin.
- A disease with an unfavorable prognosis - osteogenesis imperfecta - like others, is manifested by significant weakness of the ligamentous apparatus. But in addition to weak ligaments, osteogenesis imperfecta is characterized by frequent bone fractures, hearing loss and other serious consequences.
Transient joint hypermobility
Some “looseness” of the joints may occur during pregnancy. Although pregnancy is not a disease, hormonal changes are observed in a woman’s body.
These include the production of relaxin, a special hormone that increases the elasticity and extensibility of ligaments.
In this case, the good goal is to prepare the pubic symphysis and birth canal for stretching during childbirth. But since relaxin does not act on a specific joint, but on the entire connective tissue, hypermobility also appears in other joints. After giving birth, she safely disappears.
Symptoms of hypermobility
All symptoms associated with this pathology will be observed exclusively from the articular apparatus. People with hypermobility syndrome will have the following complaints:
- Frequent joint pain, even after minor injuries and normal physical activity. The knee and ankle joints are especially affected by this syndrome.
- Dislocations, subluxations of joints.
- Inflammation of the membrane lining the joint cavity - synovitis. It is important that you can always notice a connection with stress or injury.
- Constant pain in the thoracic spine.
- Curvature of the spine - scoliosis. Even with normal loads - carrying a bag on your shoulder, sitting incorrectly at a table - scoliosis will appear early, and the curvature will be significant.
- Muscle pain.
Diagnostics
Hypermobility syndrome is recognized by an attentive doctor at the patient’s first visit. It is enough to ask him carefully about his complaints, their connection with the load and carry out the simplest diagnostic tests:
- Ask to touch the inside of your forearm with your thumb.
- Offer to bring the little finger to the outside of the hand.
- Check whether a person, bending over, can rest his palms on the floor. The legs remain straight.
- See what happens when you straighten your elbows and knees. With hypermobility syndrome, they hyperextend in the other direction.
Additional examinations are needed if the doctor suspects a specific connective tissue disease. Then the following methods are used:
- radiography;
- CT scan;
- biochemical blood test;
- consultations with related specialists - cardiologists, rheumatologists, ophthalmologists.
You should always remember that joint mobility is only one symptom of connective tissue disease. And all the organs of which it is a part will suffer.
And often such patients have complaints from the heart, vision, headaches, fatigue, muscle weakness, and tinnitus.
Treatment
There is no method that would eliminate the cause of hypermobility syndrome. But this does not mean that such people are left without medical care. Therapy is mainly aimed at getting rid of complaints.
For severe joint pain, anti-inflammatory drugs (Nimesulide, Revmoxicam) are used.
In cases where the joints are very mobile, orthoses are used. They help weak ligaments hold joints together. Physical therapy gives good results. Its peculiarity is the training and strengthening of muscles with a fixed joint - isometric exercises. In this case, the muscles, like the orthoses, will act as a limiter.
It is important for people with hypermobility syndrome to remember that the severity of their condition directly depends on their lifestyle. By exercising, avoiding injuries, and following medical recommendations, the likelihood of complications is significantly reduced. And the quality of life practically does not suffer.
How to forget about joint pain?
- Joint pain limits your movements and full life...
- You are worried about discomfort, crunching and systematic pain...
- You may have tried a bunch of medications, creams and ointments...
- But judging by the fact that you are reading these lines, they did not help you much...
Crunching in the joints of a child
If a child has cracking joints in his arms and legs, parents are advised to pay attention to this and monitor the development of the situation. The main causes of crunching in infants and toddlers are insufficient development of the musculoskeletal system and active growth. In most cases, the joints hurt and click until a certain age: this is not dangerous and will go away as you grow older. If the situation persists for more than 3 years, you should consult a doctor.
Why do my child's joints crack?
Sometimes the baby’s joints crackle, but this is not a deviation and is associated with physiological characteristics:
- Insufficient production of specific joint fluid. This condition is common in one-year-old babies. The fact is that in the first year and a half the child’s skeleton is actively growing, but the body may not immediately adapt to such changes. The joints in the knees, legs, elbows, shoulders and other places increase in size, but the synovial fluid is secreted less than expected until the body adapts to the new condition. Therefore, parents notice the crunching of the joints, and it seems as if they are creaking like an elderly person.
- Immaturity of the muscular-ligamentous apparatus. Due to weak ligaments and high joint mobility, you can hear the knees, shoulders, and elbow joints crunching. In this case, you don't need to do anything. When the baby grows up, the clicking symptom will disappear on its own.
- Concentration of air bubbles in the joint fluid. Sometimes behind the kneecap of the leg or in the hip joints there is a strong creaking due to the bursting of air bubbles. This symptom is typical for a 6-12 month old baby, but over time the crunching sensation will disappear.
If such symptoms are observed in children under one year of age, then special treatment will not be needed. To prevent your baby's bones from creaking, it is worth including in your diet dishes containing calcium, phosphorus, folic acid, and B vitamins. Over the course of several months, the crunching in the joints will begin to disappear, but if the situation does not normalize and the symptom becomes more pronounced, you should show your baby to the doctor .
The main causes of crunching in an infant
In a baby during the first month of life, cracks in the hip joint and other joints are often a consequence of the immaturity of the musculoskeletal system. However, such a symptom can also mean the development of more dangerous complications in the body, the most common of which are:
- reactive or juvenile arthritis;
- dysplasia affecting the hip and shoulder joints;
- rheumatism;
- pathological mobility of the articular joint.
Return to contents
Why does a crunch appear in teenagers?
Often, the causes of such a symptom are not associated with dangerous disorders and are physiological.
During the period of maturation and growth of bone tissue, an imbalance is observed in the body, as a result of which the amount of synovial fluid secreted is not enough to lubricate the actively forming and growing joints. But similar symptoms are also provoked by pathological diseases:
Dangerous symptoms to watch out for
If parents notice that a month-old baby’s joints on the leg, arms and large joints are cracking unnaturally, and at the same time the baby is anxious and behaves uncharacteristically, it is necessary to visit a pediatrician. The following symptoms should also alert you:
Pathological crunching of the joints in a child causes pain, swelling, temperature, changes in gait, and deforms the limbs.
- joints move and move apart with difficulty;
- pronounced, constant crunching, which intensifies with physical activity;
- while moving, the child becomes painful, he cries and cannot calm down for a long time;
- swelling and redness have formed at the site of the greatest crack;
- the temperature of the skin around the sore spot is higher than normal;
- the child lags behind his peers in height and weight;
- gluteal folds are not placed symmetrically;
- shortening of the lower limb is observed.
Parents should be especially alert to a pronounced click in the hip joint, because such a sign is characteristic of a congenital pathology called dysplasia. It is important to diagnose the disease in an infant, because in this case, drug treatment will give maximum results. In adulthood, the pathology leads to serious consequences, and the prognosis for a full recovery worsens.
Diagnostic measures
If the baby's joints are cracking and the condition worsens, it is necessary to consult an orthopedist and undergo a series of diagnostic measures. The examination begins in the doctor's office, who checks the knees, elbows, shoulders and hips. Next, the doctor carries out manipulations, thanks to which it will be possible to determine the symptom of slipping. The child is placed on the couch, the doctor bends the knee and hip joint, then abducts the hips evenly in both directions. If there is no pathology, the hips touch the couch without difficulty, and when the baby has a dislocation, the head of the articular joint slides into the acetabulum.
To make an accurate diagnosis, laboratory and instrumental diagnostics are performed. The baby needs to undergo a general blood and urine test, and undergo an ultrasound of the joints and heart. If the diagnosis is confirmed and the infant has congenital joint problems, a treatment regimen is prescribed. If you start treatment during childhood, you can often avoid complications. At an older age, it will be more difficult to get rid of the disorder.
What treatment is prescribed?
When a baby has cracking joints on the legs or arms, and the cause of this disorder is a pathological condition, a special treatment regimen is prescribed. If rheumatism or an infectious complication is diagnosed, antibacterial therapy is carried out using non-steroidal anti-inflammatory drugs and glucocorticoids. When the knee crunches due to a weak muscular-ligamentous system, it is necessary to undergo a course of therapeutic massage and special exercises that will help strengthen and normalize muscle tone.
If there is a lack of specific fluid in the joint, the doctor will recommend that parents monitor the baby’s drinking regime. A special menu, which is important to enrich with vegetables, fruits, dairy and fermented milk products, meat, fish, and eggs, will help normalize the condition. By following all the doctor’s recommendations, you will be able to solve the problems without consequences, and you will need to resort to heavy medications only in extreme cases.
How to prevent a violation?
If parents notice that their newborn’s bones are crunching, and this symptom worries them, then the first preventive measure to avoid complications is a timely visit to the pediatrician. If no serious pathologies are identified, it is recommended to enroll your baby in a course of therapeutic massage to improve the condition of joints and bone tissue. For an older child, it is important to monitor nutrition, drink plenty of fluids, and remove harmful foods from the diet. It is also important from childhood to get accustomed to an active pastime, to harden yourself, and to play sports.
Joint hypermobility is a condition that is most often considered a feature of the body, and only occasionally can act as a pathology. In some cases, this may be a hereditary feature, especially if no other pathologies are detected, or a genetic disease in which joints and cartilage become more extensible, but also more fragile, which often leads to their rupture or other injuries. Therefore, hypermobility is a significant contraindication for sports that require flexibility and stretching, as there is a risk of injury.
Accompanying illnesses
Joint hypermobility in children is not only pathological joint mobility, but also some other diseases that may be concomitant. This may include:
- Increased skin elasticity.
- Heart valve defects.
- Hernias of internal organs.
- Prolapse of internal organs.
- Formation of large hemorrhages after minor bruises.
- Early onset and rapid progression of varicose veins.
- Frequent fractures.
- Hypotonicity syndrome, which is expressed in the fact that children begin to walk and sit late.
- Myopia.
- Strabismus.
All of the listed symptoms or the presence of several of them indicate that hypermobility is a hereditary pathology that requires treatment, and not a feature of connective tissue. Therefore, in such cases, joint hypermobility syndrome requires careful diagnosis and immediate treatment.
Clinical picture
 The main symptom that most often attracts attention is pain in the joints and muscles, which appears when weather conditions change, during emotional experiences. Such people often consult a doctor with dislocations and subluxations, which are chronic and can even occur on their own. The ankle and shoulder are most often affected.
The main symptom that most often attracts attention is pain in the joints and muscles, which appears when weather conditions change, during emotional experiences. Such people often consult a doctor with dislocations and subluxations, which are chronic and can even occur on their own. The ankle and shoulder are most often affected.
Another characteristic symptom is long-term inflammatory processes in the joints and surrounding tissues, for example, or, occurring against the background of intense physical activity.
Painful sensations can appear not only in large joints, but also in the legs, while patients experience varying degrees of flat feet, which leads to curvature of the legs and the development of premature osteoarthritis. In this case, the spine also suffers, in which pain, deformation, and disc herniation are diagnosed. All this often appears in women without hypermobility syndrome, but in the latter case, the first signs of the disease begin to appear at a very early age, which is not typical for diseases of the spine.
In newborns in the first weeks of life, joint hypermobility syndrome is almost impossible to detect, which is associated with physiological muscle hypertonicity. Later, this syndrome occurs equally often in both boys and girls, but then the situation changes, and during puberty the disease is diagnosed almost only in girls. As the child grows and bone and cartilage tissue matures, this disease goes away on its own, without any treatment, but sometimes this does not happen, and then active treatment is required throughout almost the entire life.
Criteria for evaluation
To make a diagnosis of “joint hypermobility syndrome,” which can be seen in the photo, there is a test, after which a final diagnosis is made and treatment is prescribed. The test is carried out according to the following parameters:
- Flexion of the fifth finger in both directions.
- Flexion of the first finger towards the forearm while flexing the wrist joint.
- Hyperextension of the elbow by more than 10 degrees.
- Hyperextension of the knee by more than 10 degrees.
- When you lean forward and your knees are fixed, your palms rest completely on the floor.
Conservative therapy
Treatment of joint hypermobility should be strictly individualized. It is very important to eliminate factors that can lead to injuries, so children should not take part in team sports or attend sports clubs. It is necessary to ensure that when moving the child does not experience pain in the joints, and when pain occurs, loads, including physical ones, must be strictly dosed.
For persistent and persistent pain, wearing elastic orthoses is required. Prevention of flat feet is very important, and at the first signs of manifestations of this disease, immediate treatment is required.
Exercises are very useful, but they must be carried out under the strict supervision of a specialist and must be gentle. Since the disease is genetic, it cannot be cured, but the general condition can be significantly improved.