What is cardiomyopathy? Description of the disease, its types. Prognosis for different types of cardiomyopathy
Among the many pathologies of the heart, cardiomyopathy is distinguished. Such a pathology occurs for no apparent reason and is accompanied by dystrophic lesions of the heart muscle. In this article we will tell you what kind of anomaly it is, why it occurs and what characteristic features it has. We will also consider the main methods of its diagnosis and treatment.
Description of pathology
Many patients, after being diagnosed with cardiomyopathy, do not even suspect what it is. In cardiology, there are many heart diseases that occur against the background of an inflammatory process, the presence of a malignant neoplasm, or coronary disease.
Primary cardiomyopathy is not associated with such phenomena. This is a general definition for pathological conditions of the myocardium of uncertain etiology. They are based on the processes of dystrophy and sclerosis of cardiac cells and tissues.
Types of primary cMP
Doctors make such a diagnosis to the patient under the following circumstances:
- During the examination, signs of dystrophic damage to the heart muscle were found.
- After the analyzes were not revealed:
- congenital anomalies of the heart;
- heart valve defects;
- systemic lesions of the coronary vessels;
- pericarditis;
- hypertension.
- There are unpleasant symptoms: heart enlargement, arrhythmia, progressive heart failure.
Cardiomyopathy is a group of cardiac pathologies of idiopathic origin. They are characterized by the presence of severe myocardial damage in the absence of congenital or acquired cardiac anomalies.
Why does it occur and how does it develop?
Why does cardiomyopathy appear? Its reasons can be very different. It all depends on what kind of cardiomyopathy it is - primary or secondary. Primary may be congenital, acquired or mixed. Congenital develops during fetal development, when abnormalities of the heart cells occur. Here an important role is played by:
- heredity;
- gene anomalies;
- mother has bad habits;
- stress transferred during pregnancy;
- malnutrition of a woman during gestation.
Causes of pathology
Acquired or mixed cardiomyopathies occur due to:
- pregnancy;
- myocarditis;
- damage by toxic substances;
- hormonal disorders;
- immune pathologies.
Secondary cardiomyopathy develops against the background of certain diseases. Among them:
- Genetic disorders (accumulation of abnormal inclusions between heart cells).
- Presence of tumors.
- Drug, toxic or alcohol poisoning;
- Violation of metabolic processes in the myocardium. It arises due to:
- menopause;
- malnutrition;
- excess weight;
- endocrine disorders;
- diseases of the digestive system.
Most often, this pathology is observed in adults. But it can also occur in children, especially due to physiological causes - due to a violation of the development of heart cells during growth and development.
Symptoms
Often the symptoms of the disease are hidden. Patients can live a long life without suspecting that they have a dangerous pathology. But at the same time, it develops and provokes the occurrence of serious complications. The initial stage of cardiomyopathy is easily confused with other diseases. Its characteristic features:
- shortness of breath (with strong physical exertion);
- heartache;
- general weakness;
- dizziness.
Symptoms of the disease
Subsequently, more pronounced and dangerous signs are added to such symptoms. Among them:
- increased blood pressure;
- fast fatigue, lethargy;
- pallor of the skin, the appearance of its cyanotic hue;
- swelling (especially of the lower extremities);
- severe chest pain;
- increased heart rate, arrhythmia;
- periodic loss of consciousness.
Symptoms, as a rule, depend on the type of cardiomyopathy, as well as on the severity of the pathological condition. To determine the disease, you need to consult a doctor, undergo a thorough examination.
Classification and characteristics
There are many types of cardiomyopathy. Depending on the causes, the following forms of pathology are distinguished:
- ischemic (occurs due to ischemic damage to the heart cells);
- dysmetabolic (associated with impaired metabolic processes);
- dishormonal (develops due to hormonal disruptions, for example, in women during pregnancy or after menopause);
- genetic;
- alcoholic;
- medicinal or toxic;
- takotsubo or stress (it is also called broken heart syndrome).
ILC classification
Most doctors divide cardiomyopathy into the following types to determine the anatomical and functional changes in the heart muscle:
- dilatational;
- hypertrophic;
- restrictive;
- arrhythmogenic right ventricular.
They have their own developmental features and specific characteristics. Let's consider each of them in more detail. Thus, the dilated or congestive form most often occurs under the influence of infection, toxic damage, metabolic, hormonal and autoimmune failures.
Dilated form
It is manifested by signs of right ventricular and left ventricular failure, pain in the heart, which is not relieved by nitrate-containing drugs, palpitations and arrhythmia. She is characterized by:
- enlargement of the heart chambers;
- hypertrophy;
- deterioration of the contractile function of the heart.
There is also a deformity of the chest, which is called the heart hump. With this form, the patient experiences attacks of cardiac asthma, pulmonary edema, ascites, swelling of the jugular veins, and an enlarged liver.
Hypertrophic IMP
The main cause of the hypertrophic form of the disease is an autosomal dominant type of hereditary pathology, which occurs more often in men at different ages. She is characterized by:
- myocardial hypertrophy (may be focal or diffuse, symmetrical or asymmetric);
- a decrease in the size of the ventricles of the heart (with or without obstruction - a violation of the outflow of blood from the left ventricle).
The specificity of this form is the presence of signs of aortic stenosis in the patient. Among them:
- cardialgia;
- increased heart rate;
- dizziness, weakness, loss of consciousness;
- dyspnea;
- excessive pallor of the skin.
This pathology often causes sudden death of the patient. For example, athletes during training.
In the restrictive form, there is increased rigidity (hardness, inflexibility) of the myocardium and a reduced ability of the heart walls to relax. In this case, the left ventricle is poorly filled with blood, which leads to thickening of the walls of the atria. The contractile activity of the myocardium is preserved, the heart is not prone to hypertrophy.
Restrictive cardiomyopathy goes through several stages of development:
- Necrotic. It is manifested by the development of coronary lesions and myocarditis.
- thrombotic. At this stage, the endocardium expands, fibrous deposits appear in the cavity of the heart, and thrombi appear in the myocardium.
- Fibrotic. At the same time, fibrosis of myocardial tissues spreads, obliterating endarteritis of the coronary arteries occurs.
This form is characterized by the presence of signs of severe circulatory failure. This is manifested by shortness of breath, weakness, swelling, ascites, enlargement of the liver, swelling of the jugular veins.
Restrictive type of pathology
Arrhythmogenic right ventricular cardiomyopathy is a fairly rare pathology that presumably develops as a result of a hereditary predisposition, apoptosis, exposure to a viral infection, or chemical poisoning. It is characterized by the replacement of heart cells with fibrous tissue. Against the background of such a disease are observed:
- extrasystole or tachycardia;
- ventricular fibrillation;
- atrial fibrillation;
- tachyarrhythmias.
Diagnostic methods
To identify the disease, you should visit a cardiologist. To begin with, he will conduct an examination and interview, examine the patient's medical record. After that, a thorough examination should be carried out to determine the form and severity of the pathology, possible causes. Often the patient is prescribed:
- blood test for hormones;
- blood chemistry;
- ultrasound examination of the heart (determine the size of the heart and its other parameters);
- electrocardiography (fixes signs of myocardial enlargement, heart rhythm disturbances and its conduction);
- x-ray of the lungs (reveal dilation and enlargement of the myocardium, possible congestion in the lungs);
- echocardiography (determination of myocardial dysfunction);
- ventriculography;
- sounding of the cavities of the heart for morphological research;
- Magnetic resonance imaging.
Such diagnostics is carried out only in special medical institutions. It is prescribed by the attending physician in the presence of relevant indications.
Methods of treatment
Cardiomyopathy is difficult to treat. It is important that the patient complies with all doctor's instructions. There are several methods of therapy.
Medical therapy
This is a treatment with the help of special medications. The following are often prescribed for such a pathology:
- beta-blockers (Atenolol, Bisoprolol) improve cardiac work, reduce its need for oxygen;
- anticoagulants (reduce blood clotting) to prevent the development of thrombosis (Heparin, Warfarin);
- drugs that lower blood pressure (ACE inhibitors - Captopril and analogues);
- antioxidants (Carvedilol);
- diuretics (furasemide) to reduce swelling and reduce pressure.
Any medication should only be taken as directed by a doctor. Self-medication can be detrimental to health or even lead to death.
Surgical intervention
If the medications do not have the desired effect, and the patient is getting worse, surgical treatment may be used. In this case, there are such methods:
- implantation of a pacemaker (in violation of the heart rhythm);
- defibrillator implantation;
- donor heart transplant.
The last procedure is a very complex and dangerous operation. It is carried out if other methods do not help and the patient dies.
Prevention of complications
When cardiomyopathy occurs in a patient, the risk of negative complications increases. To avoid them, you should follow these recommendations:
- lead a healthy lifestyle;
- avoid excessive stress on the heart;
- avoid stress and negative emotions;
- stop smoking, do not abuse alcoholic beverages;
- eat properly;
- observe the sleep and rest regimen.
Prevention of cardiovascular diseases
If the pathology is secondary, that is, it has arisen against the background of a particular disease, then the patient should constantly monitor his state of health. He must also take courses of treatment and follow the doctor's instructions.
Forecast
It is very difficult to predict the disease. As a rule, with severe myocardial damage - chronic heart failure, heart rhythm disturbances (arrhythmia, tachycardia), thromboembolic complications - death can occur at any time.
Also, the form of pathology affects life expectancy. If congestive cardiomyopathy is detected, then the patient is given no more than 5-7 years. A heart transplant increases a person's life by an average of 10 years. Surgical intervention for aortic stenosis often ends in death (more than 15% of those operated on die).
It should also be remembered that women with this diagnosis should not plan the birth of a child. It is highly likely that the expectant mother will die without even waiting for childbirth.
To date, there are no specific preventive measures that can protect against the development of the disease.
Cardiomyopathy is a pathological condition of unknown origin. It can be both congenital and acquired.
Treatment of the disease is a long process that does not always give a positive result.
Source: https://simptomov.com/kardio/kardiomiopatiya/

Cardiomyopathy is an understudied pathology of the heart muscle. Previously, one could hear such a name - myocardiopathy (from a combination of words: myocardium and pathology). But this free interpretation is not applied today, since cardiomyopathy occupies two sections in ICD-10 - I 42 and I 43.
It is more logical to use the name of cardiomyopathy, that is, in the plural, since even in the ICD-10 in two sections there are a dozen and a half varieties that differ both in signs and in causes.
Note that pathology is extremely unfavorable in the prognosis. There is a high chance of complications that can lead to sudden death.
Important. The group of cardiomyopathy combines pathologies that are selective deformation of the heart muscle (myocardium).
The essence of selectivity is that only the heart muscle changes structurally and functionally, but the important parts of the body associated with it, for example, the coronary arteries, the valvular apparatus of the heart, do not undergo changes.
Advances in the understanding of cardiomyopathies were marked by the 1980 classification, which made reference to the unknown origin of cardiac muscle pathologies. And only in 1996, by the decision of the international society, a cardiologist put an end to the definition of cardiomyopathies as various myocardial diseases, which are characterized by cardiac disorders.
The diseases are characterized by pathological changes in the myocardium, which are manifested by heart failure, arrhythmia, fatigue, swelling of the legs, and a general deterioration in the functioning of the body. There is a considerable risk of developing serious cardiac arrhythmias with a fatal outcome.
The disease affects people of any age group, regardless of gender. Cardiomyopathies are divided into several types depending on the specific effect on the heart muscle:
- hypertrophic,
- dilatational,
- arrhythmogenic,
- pancreatic,
- restrictive.
All types of the disease can be divided into primary (the cause is unknown) and secondary cardiomyopathy (hereditary predisposition or the presence of a number of diseases that violate the body's defenses). According to statistics, dilated and restrictive cardiomyopathies are the most common.
Hypertrophic cardiomyopathy is a thickening of the walls of the left ventricle (myocardial damage), while the cavities remain the same or decrease in volume, which significantly affects the heart rhythms.
A decrease in contractile function occurs due to the thickening of the walls of the chambers due to inclusions of scar tissue, which does not have the functionality of heart muscle cells. As a result of a decrease in the ejection of blood, its remnants accumulate in the ventricles. Congestion occurs, which leads to heart failure. DCM due to congestion has received another name - congestive cardiomyopathy.
It is believed that up to 30% of cases of diseases are caused by genetic factors in the development of dilated cardiomyopathy. Viral nature is fixed by statistics in 15% of cases.
The situation with uneven thickening of the walls of the cavities of the heart has its own name - cardiomegaly. Otherwise, this pathology is called “huge heart”.
As a variant of this form of pathology, ischemic cardiomyopathy is diagnosed.
It is characteristic that with this diagnosis there are multiple atherosclerotic vascular lesions and heart attacks may have been transferred (after all, the scar tissue in the heart muscle came from somewhere).
Important. Ischemic cardiomyopathy is not similar to coronary artery disease with its retrosternal pain, but is based on the expansion of the walls and on early heart failure. The main hit (nine out of ten!) falls on men under the age of 50 or so.
In addition, it should be noted that congestive heart failure (i.e., congestive cardiomyopathy) is often the cause of sudden death.
Statistics state that DCM is 60% more likely to affect men than women on gender grounds. This is especially true for the age groups from 25 to 50 years.
In general, the cause of the disease can be:
- any toxic effect - alcohol, poisons, drugs, anti-cancer drugs;
- viral infection - common flu, herpes, Coxsackie virus, etc .;
- hormonal imbalance - protein deficiency, vitamin, etc .;
- diseases that cause autoimmune myocarditis - lupus erythematosus or arthritis.
- heredity (family predisposition) - up to 30%.
Particular attention should be paid to a subspecies of DCMP, which is called alcoholic cardiomyopathy. The reason for the development of this specific subspecies is exposure to the poison ethanol.
Although this fact concerns the abuse of alcohol, but the very concept of "abuse" has no clear boundaries. For one organism, one hundred grams is enough to determine abuse.
And for another, this volume is “what a pellet for an elephant.”
Attention! Statistics claim that the alcoholic form of dilatation in the total volume of all cases of dilated cardiomyopathy takes 50%. Moreover, chronic alcoholics will never recognize addiction as the cause of the disease.
In addition to the general symptoms, the alcoholic form is characterized by:
- discoloration of the face and nose towards red,
- yellowing of the sclera,
- occurrence of insomnia
- night choking,
- hand tremor,
- increase in excitability.
Restrictive cardiomyopathy
In a large circle of blood circulation, stagnation of blood in the veins is formed, even with minimal physical exertion, shortness of breath and weakness, swelling appear, tachycardia and a paradoxical pulse appear. Cardiohemodynamics is disturbed (the elastic stiffness of the ventricles increases sharply), as a result of which, intraventricular pressure in the veins and pulmonary artery increases sharply.
Causes of Primary Cardiomyopathy
The reasons that provoke the development of this disease are quite different. Primary pathology is often caused by the following factors:
- autoimmune processes that lead to self-destruction of the body. Cells in relation to each other act as "killers". This mechanism is triggered both by viruses and by some pathological phenomena that progress;
- genetics. At the level of embryonic development, there is a violation of the laying of myocardial tissues caused by nervousness, malnutrition or smoking, or mother's alcoholism. The disease develops without symptoms of other diseases due to cardiomyocytes acting on protein structures involved in the contraction of the heart muscle;
- the presence in the body of a large number of toxins (including nicotine and alcohol) and allergens;
- poor functioning of the endocrine system;
- any viral infections;
- cardiosclerosis. Connecting fibers gradually replace the cells of the heart muscle, depriving the walls of elasticity;
- previously transferred microcarditis;
- a general disease of the connective tissue (diseases that develop with weak immunity, causing inflammatory processes with the appearance of scars in the organs).
- cumulative, which is characterized by the formation of pathological inclusions in or between cells;
- toxic, arising from the interaction of the heart muscle with anticancer drugs and getting damaged at the same time; frequent use of alcohol for a long time. Both cases can cause severe heart failure and death;
- endocrine, which appears in the process of metabolic disorders in the heart muscle, losing contractile properties, wall dystrophy occurs. Occurs during menopause, diseases of the gastrointestinal tract, diabetes;
- alimentary, arising from malnutrition with diets, starvation and a vegetarian menu.
Cardiomyopathy. Symptoms and signs
The symptoms depend on the type of the disease itself. With the development of dilated cardiomyopathy, there is an increase in all four cavities of the heart, expansion of the ventricles and atria. Because of this, the heart muscle cannot cope with the stress.
Signs of DCMP. Even with minimal physical exertion, shortness of breath occurs; legs become swollen, there is a feeling of fatigue; the area around the mouth, wings of the nose, earlobes, fingers, ankles and feet become bluish.
With hypertrophic cardiomyopathy, thickening of the walls of the heart occurs, which entails a decrease in the size of the heart cavities themselves. This affects the ejection of blood with each contraction. Its amount is much less than necessary for normal blood circulation in the body.
Signs of hypertrophic cardiomyopathy. There is tachycardia, pain in the heart, pale complexion, constant fainting, weakness and shortness of breath.
With the development of restrictive cardiomyopathy, scarring of the heart muscle occurs. The heart can never relax, its work is disturbed.
Signs of restrictive cardiomyopathy. The skin becomes bluish in color, shortness of breath attacks become more frequent, swelling occurs not only in the limbs, but also in the abdomen, the liver undergoes an increase in size. This type of cardiomyopathy is considered the most severe and rare.
X-ray, echocardiography, Holter mount, electrocardiography and physical examination are used. Each of these methods has its own advantages and disadvantages. All procedures are absolutely painless and do not pose any danger. Unfortunately, how accurate the diagnosis will be depends on the qualifications of the specialist, since due to the similarity of symptoms, doubts can arise about the type of CMP.
To understand the degree of damage to the heart, a physical examination (palpation, percussion, diagnostic procedures) is most often used. But, often, this is not enough to make a diagnosis, so additional methods are included in the examination complex.
An electrocardiogram is a graphical representation of the work of the heart. With a detailed study by an experienced doctor, its decoding makes it possible to make an accurate diagnosis.
The most modern method is diagnostics using echocardiography. This method gives a clear visibility of the state of the heart, which allows you to make a clear diagnosis without additional research - what kind of cardiomyopathy the patient has. The method is suitable for absolutely everyone, even pregnant women and children. You can repeat it many times.
Radiography involves the use of x-rays. It does not require preparation and is relatively cheap. But the diagnosis by this method is not shown to everyone due to the effects of rays on the human body. Yes, and the information received is incomplete and compressed, so an additional examination is prescribed.
Holter monitoring is an examination using a device that must be worn on the body for a whole day without removing it. It does not cause inconvenience, as it weighs less than a kilogram. Diagnosis, by and large, depends on the patient himself.
He must keep a written record of all physical activity, medication, pain that occurs, etc. In addition, forget about hygiene procedures for the duration of the examination. But this method is the most accurate.
During the day, detailed performance of the heart muscle is viewed.
Treatment
Therapy methods are relatively the same, focused on the elimination of the underlying disease.
A specialist can prescribe a course of therapy that will support the overall functioning of the heart, slow down further development and improve the condition of the myocardium. The patient needs constant monitoring by a cardiologist, periodically inpatient treatment and adherence to the rules of a healthy lifestyle (moderate physical activity, proper nutrition, giving up bad habits, etc.).
Therapeutic treatment directly depends on the stage of development of the disease. If this is a primary ailment, it is necessary to restore the normalization of the work of the heart muscle and exclude heart failure.
With a secondary disease, the main task is to treat the underlying disease. For example, when an infection is affected, antibiotics and anti-inflammatory drug treatment are initially prescribed.
And only after that - the restoration of the activity of the heart.
If the disease is too advanced, surgery (heart transplantation) is required. Surgery for the treatment of cardiomyopathy is relatively rare. It is used only in the case of a secondary form of the disease, with the elimination of the underlying disease. An example is heart disease.
Forecast
Cardiomyopathy in terms of prognosis is extremely unfavorable. The resulting heart failure will steadily progress. The danger is that the pathology may not manifest itself for a long time. Yes, there seem to be some unpleasant sensations, but they can often be attributed to domestic stress, fatigue during work, etc.
However, arrhythmic or thromboembolic complications gradually occur, which can lead to sudden death at a fairly young age.
The statistics are relentless on dilated cardiomyopathy. Once diagnosed, the five-year survival rate is only 30%. Although systematic treatment allows you to stabilize the condition for an indefinite period.
Extremely important! Even when diagnosing DCMP, do not let the treatment take its course! You can live long enough and in conditions of systematic treatment.
Heart transplantation can give good results in terms of survival. Cases of exceeding 10-year survival after such operations have been recorded.
Subaortic stenosis in hypertrophic cardiomyopathy has not proven itself very well. His surgical treatment carries high risks. According to statistics, every sixth patient dies either during or after surgery in a short time.
Very important! Women diagnosed with cardiomyopathy pregnancy is contraindicated because of the high risk of maternal mortality.
Source: http://serdcet.ru/kardiomiopatiya.html

From this article you will learn: what is cardiomyopathy, what it can be. Why experts perceive such a disease differently, symptoms, whether it is possible to fully recover.
Cardiomyopathy can be understood as any violation of the structure of the heart in the form of a pronounced increase in size (cardiomegaly), leading to the inability of the myocardium to perform its function - to heart failure. But this definition, provided by the international classification of diseases, is not entirely correct. Indeed, in this case, most cardiac pathology can be considered as cardiomyopathy.
Many cardiologists perceive as this pathology only those cases of heart failure that are not similar to any other myocardial disease. About 50% of such patients in the early stages do not show any cardiac complaints at all, or they are minimally expressed (periodic chest discomfort, general weakness).
In the remaining 50%, the disease is detected at the stage of pronounced rearrangements in the heart or complications - shortness of breath during exertion or even at rest, swelling of the legs and the whole body, brain disorders. In this regard, patients cannot perform physical activity or even go outside the room. A fatal outcome due to heart failure against the background of cardiomyopathy is also possible.
The pathology can be completely cured only by a heart transplant. All other treatment under the supervision of a cardiologist is aimed at slowing the progression of changes in the myocardium and circulatory failure.
Description of the disease, its types
According to modern concepts, cardiomyopathy is a group of causeless dystrophic lesions of the heart that are not associated with inflammation (carditis), circulatory disorders, hypertensive and tumor degeneration of the myocardium.
With this disease, the heart loses its normal structure, increases in size (cardiomegaly), becomes flabby and unable to pump blood.
As a result, there are manifestations of circulatory failure throughout the body.
All this means that:
- true cardiomyopathy - only those changes in the myocardium that are not like any other heart disease;
- the disease is a separate idiopathic pathology - one whose causes are difficult or impossible to establish;
- the main manifestation of the disease is heart failure caused by pronounced structural changes in the myocardium (thickening, thinning, destruction);
- treatment is mainly aimed at reducing the manifestations of circulatory failure and improving myocardial nutrition.
The described features characterize the primary (true) form of cardiomyopathy. It is relatively rare (no more than 5% of cardiac pathology), but mainly among people of working age (30–55 years).
Different specialists have different attitudes to this diagnosis: some use it in everyday practice, others consider it wrong.
This is due to the fact that secondary myocardial changes due to cardiac and non-cardiac pathology, in fact, are its natural manifestation. Therefore, it is advisable to isolate secondary cardiomyopathy in cases where the symptoms of heart damage are equally pronounced with the underlying pathology.
Depending on the causative pathology, secondary cardiomyopathy can be:
- Valvular - due to damage to the valves.
- Hypertensive - thickening (hypertrophy) of the myocardium against the background of a constant increase in pressure (it is also called a hypertensive heart).
- Inflammatory - a consequence of a transferred or sluggish inflammatory process in the myocardium.
- Metabolic (exchange) - the result of impaired metabolism in diseases of the thyroid gland, adrenal glands, the accumulation of abnormal proteins in the body.
- Toxic - changes in the heart against the background of exposure to various toxic substances (alcohol, chemicals, certain medications).
- Systemic and autoimmune - as a complication of leukemia, sarcoidosis, lupus erythematosus, scleroderma, rheumatoid arthritis and other connective tissue diseases.
- Myodystrophic and neuromuscular - a manifestation of the general pathology of muscle tissue and the transmission of nerve impulses from nerves to muscles (for example, Duchenne and Becker myodystrophy, Friedreich and Nuan ataxia syndromes).
The only diseased organ in primary (true) cardiomyopathy is the heart, and all other manifestations and complications arise as a result of its insufficiency. In the secondary form of this disease, myocardial damage, on the contrary, is due to violations of the structure and function of other organs.
What happens to the heart in different types of true cardiomyopathy
Depending on how the heart changes, primary (true) cardiomyopathy can be:
- Hypertrophic - an increase in the heart (cardiomegaly) due to thickening of the myocardium (hypertrophy of the heart muscle). Cells altered in this way are defective, since they do not receive normal nutrition, are not able to perform their function, or narrow the lumen of the vessels into which blood is ejected.
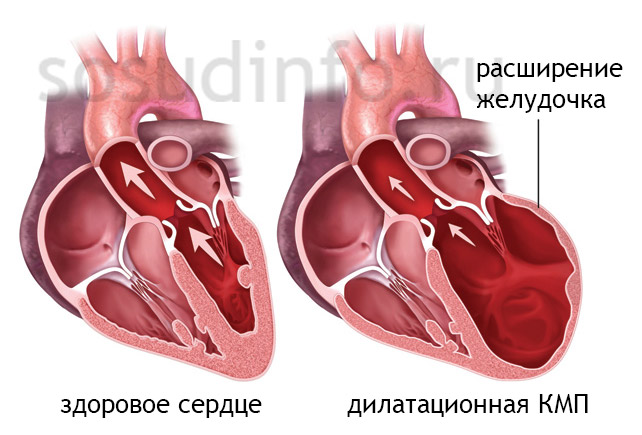
- Dilated - pronounced cardiomegaly due to thinning of the walls of the myocardium and expansion of its cavities, which is accompanied by excessive overflow of blood and the inability to pump it into the vessels.
- Restrictive - cardiomyopathy, in which there is no cardiomegaly, as the myocardium becomes dense and inelastic (incapable of stretching and relaxing), which impairs its ability to fill with blood. As a result - stagnation of blood in the veins and lack of arteries.
- Arrhythmogenic right ventricular - destruction and cicatricial replacement of the myocardium of the right ventricle, accompanied by arrhythmias (interruptions), signs of stagnation of blood in the lungs and oxygen starvation in all organs and tissues of the body.
Causes of the mysterious pathology
All the disagreements of specialists about cardiomyopathy, its insidiousness and mystery are due to the absence of reliably established causes. It arises without visible prerequisites, as if from nowhere, manifesting itself as an increase in the heart and symptoms of its insufficiency. However, some causes are still associated with pathology:
- Genetic predisposition and mutations. The structure and functioning of myocardial cells is supported by a variety of special proteins. Violation of their production (synthesis) can occur due to breakdowns (mutations) at the gene level. Therefore, the disease is transmitted between close relatives and has no obvious causes.
- Virus infection. There is a group of viruses (Epstein-Barr, Coxsackie, cytomegalovirus, hepatitis C, etc.) that, when they enter the body, do not cause a pronounced immune response and can stay in it for years and decades. Due to the fact that immune cells do not neutralize viral cells, they enter the heart, destroying the DNA of cells. As a result, they lose their structure.
- An autoimmune process is an abnormal reaction of the immune system to its own myocardial tissues. Immune cells destroy them, perceiving them as foreign. The reasons for starting such a process are very diverse (allergic reactions, infection with viruses and bacteria, genetic disorders, etc.), but it is extremely difficult to establish them.
- Idiopathic factors - causes, the origin of which cannot be established and even assumed (uncaused myocardial fibrosis).
Only in 40-50% of cases, the causes of primary cardiomyopathy can be established. In the remaining 50-60% of cases, only characteristic changes in the heart and signs of circulatory insufficiency are determined, which do not have any reasons.
Early and specific symptoms: why there are so few of them
Patients with cardiomyopathy do not show any complaints until heart failure occurs - the inability of the myocardium to pump blood.
For 2–3 to 5–7 years from the moment of onset, the disease proceeds insidiously, gradually destroying the heart. Therefore, cardiomyopathy has neither early nor specific symptoms.
They are represented by common cardiac manifestations that make you see a doctor:
- weakness and fatigue;
- discomfort and heaviness in the region of the heart;
- dizziness;
- pallor or blueness of the skin;
- swelling in the legs or throughout the body;
- an increase in the size of the abdomen;
- heart rhythm disturbances (interruptions, arrhythmia).
How and when cardiomyopathy manifests itself depends on the age of the patient, the condition of the heart and other organs. These factors reflect the body's readiness to adapt to changes in blood circulation.
The higher the adaptive capacity, the longer the asymptomatic course.
But in 60-70% of patients who do not have clinical manifestations according to ECG, ultrasound and chest X-ray, signs of the disease can be detected:
- an increase in the size of the heart;
- thickening (hypertrophy) and myocardial dystrophy;
- expansion of the cavities of the ventricles and atria;
- decrease in myocardial contractility;
- increased pressure in the pulmonary artery, pulmonary vessels and their expansion.
Click on photo to enlarge
Signs of heart failure and changes in the heart depend on the type of cardiomyopathy (described in the table).
| Who gets sick more often | Young men and women aged 30–35 | Mostly men aged 35–55 | Men and women 30–60 years old |
| How the heart has changed | Sharply increased due to the expansion of all cavities, the myocardium is thickened | Sharply increased due to thickening of the left ventricle, cavities are reduced | Not changed in size, the walls are thickened, the cavities are reduced |
| The nature of cardiac disorders | More often left ventricular failure - stagnation of blood in the lungs | According to the type of aortic stenosis - disorders of cerebral circulation | The heart does not receive and does not pump blood - pronounced stagnation |
| Main symptoms | Dyspnea Weakness Heaviness in the chest
Blueness of the skin Wheezing in the lungs Swollen neck veins cardiomegaly Swelling of the legs Silent heartbeats |
dizziness fainting Weakness Chest pain Pale skin Hypotension Strong heartbeat |
Dyspnea Weakness dizziness Vein tension Swelling of the legs Enlargement of the liver and abdomen Puffy bluish face |
| Other features | The heart is overflowing with blood, but the weakened myocardium cannot pump it. | Thickened interventricular septum - difficult to eject blood into the aorta | The walls of the heart are dense, like a shell, do not stretch or contract |
Symptoms and clinical manifestations of the most common types of cardiomyopathy - dilated, hypertrophic and restrictive - differ only slightly in mild heart failure. If it is decompensated (severe), the signs become the same in all patients due to the poor functioning of all parts of the heart (both ventricles and atria).
In addition to early circulatory failure, other complications may occur that require urgent treatment:
- Arrhythmia (atrial fibrillation).
- Thromboembolic complications - the formation of blood clots in the heart with their further separation and migration into the vessels of the lungs (PE), brain (stroke), intestines (intestinal gangrene), legs (foot gangrene).
- Heart block.
- Sudden cardiac arrest.
Diagnostic methods
Suspicion of cardiomyopathy - indication for diagnosis:
- extended ECG;
- chest x-ray;
- echocardiography;
- biochemical and complete blood count, troponins, lipid spectrum;
- chest tomography;
- catheterization of the heart cavities with a biopsy (tissue sampling for analysis).
Is it possible to heal
Cardiomyopathy is treated poorly - it cannot be cured, you can only reduce the severity of symptoms and the rate of progression of pathological changes in the myocardium. For this, cardiologists prescribe complex conservative therapy:
- A diet that excludes fatty foods of animal origin, pastry products and other foods high in cholesterol. Includes vegetables and fruits, vegetable oils, dietary meat.
- Dosed physical activity is a sparing regimen that eliminates overstrain and stress.
- Lifelong treatment with ACE inhibitors - drugs: Berlipril, Enap, Lipril or angiotensin blockers: Losartan, Valsakor.
- Taking beta-blockers: Bisoprolol, Propranolol, Carvedilol, Nebival. Their treatment is carried out under the control of pressure and heart rate (they reduce them).
- Nitrates: Nitroglycerin, Isoket, Nitro-mic, Nitro-long (contraindicated at low pressure).
- Diuretic: Trifas, Lasix, Furosemide, Hypothiazide - reduce swelling and congestion in the lungs.
- Treatment with glycosides - drugs that increase myocardial contractility: Digoxin, Strofantin.
- Metabolic therapy - improvement of myocardial nutrition: Preductal, Vitamins E and B, Mildronate, ATP.
The only possibility of a complete cure is an operation - transplantation (transplantation) of the heart, which is indicated for progressive destructive changes in the myocardium and circulatory failure.
Prognosis for different types of cardiomyopathy
With regard to the prognosis of treatment, cardiomyopathy is an ungrateful disease.
- Survival of patients for 5 years, despite treatment, with dilated and restrictive forms does not exceed 40%.
- The hypertrophic variant is more favorable - a 5-year survival rate is 60-70%, and with an early start of treatment, patients live for decades.
In general, the course is unpredictable and can take on a different character at any time.
Timely heart transplantation in young patients (before severe complications) can achieve a 10-year survival rate of 30-50%. Pregnancy is contraindicated for life. There are no methods of prevention.
No matter how severe the pathology is - use every chance for recovery!
Scientific editor: Strokina O.A., therapist, doctor of functional diagnostics. Practical experience since 2015
November, 2018.
Cardiomyopathy is a change in the heart muscle of an often unexplained cause.
The condition for the diagnosis of cardiomyopathy is absence(or exclusion after examination)
- congenital malformations,
- valvular heart disease,
- damage caused by systemic vascular disease,
- arterial hypertension,
- some rare variants of damage to the conduction system of the heart.
Cardiomyopathies are primary, when the pathological process affects only the heart, and secondary, developing as a result of any systemic disease.
There are three main types of damage to the heart muscle in cardiomyopathies, respectively,
- dilated cardiomyopathy,
- hypertrophic cardiomyopathy
- restrictive cardiomyopathy.
Such a division is usually based on an assessment of intracardiac circulation and already at the initial stage of the disease, in some cases, it allows to establish the direction of the search for a possible cause of the process. With an unidentified underlying cause of the lesion, they speak of idiopathic forms of one or another cardiomyopathy.
Dilated cardiomyopathy (DCM)
Dilated cardiomyopathy is characterized by a violation of the contractile function of the heart muscle (myocardium) with a pronounced expansion of the chambers of the heart. Its occurrence is associated with genetic factors, since there is a family nature of the disease. The observed violations of immune regulation are of no less importance.
Symptoms of Dilated Cardiomyopathy
Manifestations of dilated cardiomyopathy are determined by increasing heart failure:
- shortness of breath on exertion,
- fast fatiguability,
- swelling in the legs,
- skin pallor,
- bruising of fingertips.
The prognosis for dilated cardiomyopathy is very serious. The addition of atrial fibrillation worsens the prognosis. In the first 5 years of the disease, up to 70% of patients die, although with regular, controlled drug therapy, it is undoubtedly possible to prolong the patient's life.
Women with dilated cardiomyopathy should avoid pregnancy because the maternal mortality rate is very high with this diagnosis. In some cases, a provoking effect of pregnancy on the development of the disease was noted.
Diagnostics
Laboratory diagnostics provides little valuable data for making a diagnosis, but it is important for monitoring the effectiveness of the therapy in assessing the state of the water-salt balance, to exclude some side effects of drugs, such as cytopenia.
The main instrumental method for diagnosing all types of cardiomyopathies is ultrasound of the heart (echocardiography). In most cases, an instrumental diagnosis of dilated cardiomyopathy can be made at the first ultrasound examination.
ECG does not have specific criteria for diagnosing dilated cardiomyopathy, however, it is possible to detect various kinds of heart rhythm disturbances up to ventricular arrhythmias (better detected with daily Holter ECG monitoring), signs of stress on the left ventricle.
Radiologically, an increase in the heart is determined, and a little later, signs of venous congestion in the lungs.
Coronary angiography - to exclude ischemic causes of expansion of the chambers of the heart.
An intravital myocardial biopsy theoretically helps to exclude specific causes (viruses, amyloidosis).
The diagnosis of dilated cardiomyopathy is a diagnosis of exclusion. It is placed when all possible causes of cardiac dysfunction are excluded.
Treatment of DCM
Treatment of dilated cardiomyopathy is aimed at combating heart failure and preventing complications. In the case of acquired DCM, treatment is directed at the underlying cause.
The main efforts in therapy are aimed at improving the contractile function of the myocardium and reducing the symptoms of heart failure with the help of ACE inhibitors. You can use any of the drugs in this group, but enalapril (Renitek, Enap) is currently used more widely than others.
If there are contraindications to the use of ACE inhibitors, sartans (valsartan, losartan) are prescribed, which have the same properties.
The choice of a particular drug is determined by tolerability, blood pressure response, side effects.
An important place is occupied by the use of small doses of beta-blockers. Treatment begins with minimal doses of the drug. In case of good tolerance, the dose can be increased, observing whether signs of heart failure increase.
The use of the drug carvedilol, a beta-alpha-blocker, which has a positive antioxidant effect on the myocardium, unique for this group, is promising.
As in the treatment of heart failure caused by other diseases, the use of diuretics has traditionally been of great importance. Their effect is monitored by monitoring the patient's weight (preferably several times a week or daily), measuring the volume of urination, monitoring the electrolyte composition of the blood.
Due to the poor prognosis of the disease, patients with dilated cardiomyopathy are considered candidates for heart transplantation.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy is a disease characterized by a significant increase in the wall thickness of the left ventricle without expanding its cavity. Hypertrophic cardiomyopathy can be either congenital or acquired. The likely cause of the disease is genetic defects.
Symptoms of hypertrophic cardiomyopathy
Most often, the disease is asymptomatic or with minor symptoms. Many patients sometimes do not even suspect that they have a serious heart disease.
Manifestations of hypertrophic cardiomyopathy are determined by complaints of shortness of breath, chest pain, a tendency to fainting, palpitations.
Due to rhythm disturbances, patients often die suddenly. Hypertrophic cardiomyopathy is often found in young men who die while playing sports.
Some patients develop gradually heart failure . Sometimes, especially in the elderly, circulatory failure develops suddenly after a long favorable course of the disease for many years.
As a result of impaired relaxation of the left ventricle, a picture of heart failure is observed, although the contractility of the left ventricle remains at normal levels until the onset of the terminal stage of the disease.
The cause of circulatory disorders in hypertrophic cardiomyopathy is a decrease in the extensibility of the heart chambers (primarily the left ventricle). The left ventricle changes its shape, which is determined by the predominant localization of the area of myocardial thickening.
Diagnostics
Laboratory and instrumental methods are used to examine a patient with suspected hypertrophic cardiomyopathy.
Laboratory
1. Routine laboratory diagnostics:
- cardiac enzymes - CPK, AST, ALT, LDH),
- blood lipids,
- thyroid hormones,
- kidney and liver tests,
- electrolytes,
- uric acid.
All this allows you to identify non-cardiac conditions that can worsen the course of heart failure.
2. Blood test for the level of brain natriuretic peptide to assess the severity of heart failure. Its high rate clearly correlates with the severity of diastolic (relaxing) function of the heart.
Instrumental
The electrocardiogram is characterized primarily by signs of thickening of the left ventricle, as well as various cardiac arrhythmias.
Radiographically, the disease may not be detected for a long time, since the external contour of the heart does not change. Later, signs of pulmonary hypertension appear.
Ultrasound of the heart (echocardiography) is a reliable method for early diagnosis of this disease, since it is able to detect a change in the internal outline of the cavity of the left ventricle.
Magnetic resonance imaging MRI of the heart is a more expensive method than ultrasound, but has a higher resolution. Thanks to him, specialists receive a clearer picture and information about the structure of the organ.
Prognosis for hypertrophic cardiomyopathy
The prognosis of the disease is most favorable in comparison with other forms of cardiomyopathies.
Patients remain able-bodied for a long time (taking into account their profession). However, in these patients, cases of sudden death are recorded with an increased frequency.
The clinic of heart failure is formed quite late. The addition of atrial fibrillation worsens the prognosis. Pregnancy and childbirth with hypertrophic cardiomyopathy are possible.
Treatment
Treatment is aimed at reducing the severity of the symptoms of the disease, improving the quality of life of the patient and preventing attacks of sudden cardiac death and progression of the disease.
The most commonly used are verapamil or diltiazem. Beta-blockers are widely used, which help to reduce the heartbeat, prevent the occurrence of rhythm disturbances and reduce myocardial oxygen demand.
If rhythm disturbances (atrial fibrillation) are detected, amiodarone or sotalol is used. In the same case, prevention of thrombus formation in the left atrium is necessary, for which anticoagulants (warfarin) are administered.
There is also a surgical treatment of hypertrophic cardiomyopathy:
- excision of a part of the interventricular septum at its base;
- cauterization of the hypertrophied base of the septum with 96% alcohol using a catheter;
- in recent years, the use of a pacemaker for two-chamber permanent pacing has been recommended.
Restrictive cardiomyopathy
Restrictive cardiomyopathy is a myocardial disease characterized by a violation of the contractile function of the heart muscle, reduced relaxation of its walls. The myocardium becomes rigid, the walls do not stretch, the filling of the left ventricle with blood suffers. Thickening of the walls of the ventricle or its expansion is not observed, in contrast to the atria, which experience an increased load.
Restrictive cardiomyopathy is the rarest form; it exists both as an independent variant and with heart damage in a fairly large range of diseases that should be excluded during the diagnosis.
These are amyloidosis, hemochromatosis, sarcoidosis, endomyocardial fibrosis, Loeffler's disease, fibroelastosis, sometimes lesions of the conduction system of the heart (Fabry's disease), systemic scleroderma and others. In children, there are heart lesions due to disorders of glycogen metabolism.
Symptoms
The insidiousness of this disease lies in the fact that the patient's complaints for the first time occur only at the stage of development of heart failure, which refers to the terminal part of the disease. Usually the cause of treatment is the appearance of peripheral edema, an increase in the size of the abdomen (ascites - fluid in the abdominal cavity), swelling of the jugular veins in the neck. A little later, shortness of breath joins the clinic.
Diagnostics
On the radiograph, the heart has the usual size, but an increase in the atria and signs of blood stagnation in the pulmonary circulation are detected.
ECG changes are not specific.
Ultrasound of the heart (echocardiography) provides valuable information:
- measurement of myocardial thickness (pronounced thickening of the walls is observed in amyloidosis and a slightly smaller change in other diseases),
- enlargement of the left atrium, assessment of the pericardium (differential diagnosis from diseases of the pericardium, which can give the same symptomatology; the presence of calcifications in the pericardium excludes the diagnosis of restrictive cardiomyopathy).
Laboratory diagnosis of restrictive cardiomyopathy does not have specific signs, but is important for identifying secondary causes of heart damage.
Treatment of restrictive cardiomyopathy
Treatment seems to be a difficult task due to the late appeal of patients, the difficulty of diagnosis, and the lack of reliable methods for stopping the process. A heart transplant may be ineffective due to the recurrence of the process in the transplanted heart.
With the established secondary nature of the lesion, there are specific methods of exposure, for example, bloodletting for hemochromatosis, corticosteroids for sarcoidosis.
The rest of the treatment is symptomatic, aimed at eliminating the clinic of heart failure. In case of heart rhythm disturbances, antiarrhythmic drugs are prescribed. Anticoagulants are used to prevent thromboembolic complications.
Forecast
Patients with restrictive cardiomyopathy are disabled. The prognosis of the disease is unfavorable, mortality in 2 years reaches 50%.
Cardiomyopathy of various types: occurrence, diagnosis and treatment of the disease
Even the most inexperienced person in medicine knows that the term "cardio" is used to refer to heart ailments, and a specialist who deals with this area is called a cardiologist. However, if you disassemble the name of such a disease as cardiomyopathy in parts, then the picture will become little clearer. Translated from the Greek "cardia" - the heart, and "pathos" - suffering. But any disease of the cardiovascular system brings incredible suffering to the patient.
The abstract name of the disease is due to the fact that in modern cardiology, the varieties of cardiomyopathies are not fully understood. Therefore, it must be recognized that this general term does not hide a specific disease, but a number of signs that contribute to a pathological change in the heart muscle (myocardium) and ventricles of the heart, which leads to heart failure and.
History and classification
The old name for a group of heart muscle diseases with various causes is. The term cardiomyopathy was introduced in 1957 at the suggestion of Wallace Brigden. Although, there was no clear classification at that time. For a long time there has been confusion in the interpretation of the terminology of primary and secondary signs of cardiomyopathy. But still, the followers of Brigden developed the theme of selective deformation of the heart muscle, without affecting other anatomical regions.
An earlier classification in 1980 was characterized by understanding cardiomyopathy as a disease of the heart muscle of unknown origin. The remaining myocardial lesions, resulting in the pathology of other organs, were considered specific. The accumulated experience of cardiologists on a global scale resulted in a new classification after 16 years.
According to the latest data from the World Health Organization (WHO) dated 1996, adopted on the basis of the decision of the International Society of Cardiology, cardiomyopathy refers to various myocardial diseases associated with impaired cardiac activity.
Depending on how it is possible to determine the cause of the disease or the mechanism of its effect on the heart muscle, there are 4 forms of cardiomyopathy:
- Restrictive;
- Arrhythmogenic.

In turn, what referred in 1980 to specific diseases of the myocardium began to be denoted by the term specific cardiomyopathy:
- Ischemic;
- valve;
- Hypertensive;
- Inflammatory;
- Postpartum;
- Cardiomyopathy as a consequence of systemic and neuromuscular diseases.
Dilated cardiomyopathy
Dilated cardiomyopathy(DCMP) is a disease that manifests itself in . The thickness of the walls of the heart muscle in this case does not change, but systolic dysfunction occurs when the contractile function of the affected ventricle of the heart (left or both) decreases, contributing to the expulsion of blood. Since the release of blood decreases, and its remnants accumulate in the ventricles, it occurs, leading to. Therefore, the dilated form is sometimes referred to as stagnant.
Cardiologists say that this disease can be idiopathic (primary), the causes of which medicine is still not clear. Secondary cardiomyopathy is caused by the following factors:
- Heredity;
- Consequence of dysregulation of immune processes;
- viral origin;
- Toxic effect on myocardial damage (alcohol, drugs, heavy metal intoxication, drug intoxication);
- Diseases of the endocrine system;
- Rare cases in the last months of pregnancy or within six months after childbirth (0.5% of all cases);
- Connective tissue diseases;
- Persistent arrhythmia.
The disease has no gender and age preferences. In the case of heredity, which statistics allocate 20 - 25%, the outcome can be the most unpredictable.
The pattern of development of dilated cardiomyopathy is such that cells begin to die in various areas of the heart muscle. They don't die on their own, of course. There are good reasons for that. As a rule, these are some kind of inflammatory processes of the heart muscle, as a result of which sick cells affected by the virus become dangerous for the body, and the immune system gets rid of them.
The muscle tissue of cells is replaced by connective tissue, which does not have the properties inherent in the myocardium (elasticity, extensibility, contractile activity). Then, to cope with the pumping functions of the heart, the chambers expand, sometimes increasing several times. Working for wear and tear, trying to deliver oxygen to all organs and tissues, the heart speeds up the rhythm . In a neglected state, persistent arrhythmias can even lead to sudden death.
Condition of patients with dilated cardiomyopathy
Before the development of heart failure, DCM does not manifest itself in any special way. Symptoms of cardiomyopathy also depend on whether one or both chambers are involved in the developing pathological process. As a rule, it is the left ventricle that is the very pump on which the state of cardiac activity depends.
Oxygen deficiency will not be slow to remind you of shortness of breath, increased fatigue, increased heart rate. At the beginning of the disease, these symptoms appear only during physical exertion, but then they manifest themselves at rest. Symptoms of cardiomyopathy include dizziness, pain in the chest and under the left shoulder blade, and insomnia. Edema may appear later.
Diagnostics
If you do not delay in going to the doctor, so as not to provoke serious complications, then people with cardiomyopathy live to an advanced age. Only a specialist cardiologist can make a diagnosis, since most of the symptoms listed above can also occur with other diseases.
The main diagnostic method is ultrasound, which gives a 100% correct answer for any form of cardiomyopathy. cannot give such a clear picture of specific changes as ultrasound, and a laboratory study allows you to create a reliable picture of the general condition of the patient (vitamin deficiency, exposure to toxic substances). plays an important role when you need to find out how enlarged the cameras are.
Treatment of dilated cardiomyopathy
The approach to the treatment of DCM is not much different from the fight against heart failure. Treatment of secondary dilated cardiomyopathy is reduced to the elimination of the previous disease that led to such pathological changes. Therapy is aimed at reducing. Beta-blockers are effective. In the event of a poor prognosis, patients are offered surgical intervention, starting with valve replacement up to.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy(HCM) is an independent disease. For him characterized by thickening of the walls of the left ventricle. HCM can be either congenital or acquired. causes the walls of the ventricle to become so hard and dense that less blood than is needed enters the ventricle. At the moment of ejection of blood from the ventricle, a smaller amount is also ejected.
According to the norm, during an increase in physical activity, the release of blood should increase, which actually does not happen. At this moment, only the pressure inside the ventricle increases, which leads to an acceleration of the heart rate.

The disease is characterized by some discrepancy between the state of the coronary system, which is no different from a healthy person, and the increased mass of the myocardium itself. The lack of blood flow in the coronary arteries causes.
The disease, as in the case of dilated cardiomyopathy, is not immediately felt. However, shortness of breath and dizziness occur later. In an active state, with insufficient blood supply to the brain, fainting may occur.
Course of the disease
The left ventricle is a fairly powerful cardiac chamber, which for a long time "responsibly" bears unbearable loads, not letting the owner know about the onset of the disease. Symptoms of malaise appear already at the last stage, when the left ventricle is losing ground. There are cases when the right ventricle is affected, but extremely rarely. The septum between both ventricles suffers much more often.
The disease develops very slowly, so patients may not feel the approaching danger for decades. The picture is quite common, when already in old age "suddenly" developed heart failure. In general, when compared with other forms of cardiomyopathy, the prognosis is quite favorable, although the disease is recognized late. Only the presence of atrial fibrillation can significantly worsen a favorable prognosis.
Revealing
An experienced cardiologist may suspect the presence of signs of HCM even with careful listening to the heart rhythm. After all, those suffering from an obstructive hypertrophic form of cardiomyopathy are observed. The higher the degree of obstruction (obstruction), the clearer the murmur. Unfortunately, there are no external signs that allow to identify the disease of HCM of another form. In this case, the ECG comes to the rescue, however, cardiomyopathy in preschool children is not detected in this way.
Echocardiography is recognized as the main research method, which makes it possible to establish the level of hypertrophy. In more complex situations, when the issue of surgical intervention is being decided, medicine resorts to sounding the heart with the broadcast of the condition on X-ray television equipment.
Fighting HCM
Drug treatment is a set of drugs that allow you to activate the processes of blood filling of the ventricles of the heart (anaprilin, metaprolol, etc.). There is also a targeted fight against severe arrhythmia. But the drugs are selected by the doctor on an individual basis, since diabetes mellitus or bronchial asthma are serious contraindications. Under constant control are the pressure and pulse of the patient.
If during the examination they found themselves, then along with the above drugs, anti-thrombotic agents are used. But these drugs also require constant monitoring of the rate of blood clotting. Surgical intervention is effective when the patient has an obstructive form and drug treatment has not yielded results. As a rule, in this case, a part of the hypertrophied myocardium of the left ventricle is cut off.
Video: hypertrophic cardiomyopathy - death in absolute health
Restrictive cardiomyopathy
Restrictive cardiomyopathy(RCMP) is a disease that manifested in insufficient myocardial distensibility. It comes from the Latin "restrictio" - restriction. These limited possibilities of the myocardium lead to the fact that the ventricles suffer from a lack of blood supply, and in the future, chronic heart failure develops.

The causes of restrictive cardiomyopathy are much more difficult to establish, since this area of \u200b\u200bknowledge still requires serious study. The primary form is so rare that the luminaries of medicine doubt whether this disease should be classified as independent. It occurs in tropical countries and is usually caused by eosinophils.
These are blood cells of allergic origin. After the endured inflammatory process in the inner shell of the heart (endocardium), this shell coarsens and loses its elasticity. Sometimes there is an adhesion of the endocardium with the myocardium. Still, more often it is a secondary disease caused by malfunctions throughout the body: metabolic disorders, protein metabolism or iron.
Patient status
Initial complaints do not differ much from the cardiomyopathies listed above, however, shortness of breath, fatigue and swelling of the legs after some time lead to more severe consequences. The work of the liver is disrupted, which leads to its increase, and then dropsy in the abdomen may develop. The rhythm of the heart is so unstable that it turns into frequent fainting.
Diagnostics
A pronounced pulsation of the veins in the neck helps the doctor to make the correct diagnosis. This indicates an obstruction in the flow of blood to the heart. Heart murmurs can also be detected during the initial examination. ECG, echocardiography, magnetic resonance imaging will dot the "i". However, in controversial cases, doctors still resort to probing, because restrictive cardiomyopathy is similar in signs to pericarditis, if detected, treatment is carried out in the opposite direction. A complete clinical and biochemical analysis will not be superfluous, since the effectiveness of treatment depends on the correct diagnosis.
Treatment of the restrictive form
Treatment complicates excess fluid in the body, and then strongly acting ones are prescribed. Most of the drugs traditionally used in heart failure are of little effect in restrictive cardiomyopathy.
Depending on the affected areas, the installation of a pacemaker may lead to a positive result. If the cause is in inflammatory processes caused by diseases such as sarcoidosis or hemochromotosis, then they are treated first of all. If there is an insufficiency in the work of the atriogastric valves, then their prosthetics are available to modern medicine. When the endocardium is significantly affected, then all affected areas are surgically removed.
Arrhythmogenic cardiomyopathy
Arrhythmogenic right ventricular cardiomyopathy(AP-KMP) is a disease recognized as a rather rare phenomenon. Medical statistics claims that it occurs on average 1: 5000 and has a hereditary nature, which does not always manifest itself. Here is such a vague characterization. However, the disease is attracting more and more attention to itself from medical scientists, because for this reason young people who are actively involved in sports often die.
Perhaps the true picture of the disease is much broader, but diagnostics are not carried out today. The replacement of the right ventricle with connective or adipose tissue leads to death. Sometimes the left ventricle is also involved in the abnormal process.
The causes of AP-KMP, in addition to genetic dependence, some physicians tend to consider transferred. However, this opinion is still at the level of research. The disease occurs mainly in people under 40 years of age.
Video: death from congenital cardiomyopathy on the football field
What are the patients complaining about?
The name of the disease speaks for itself. Patients usually suffer from ventricular arrhythmias. Patients complain of paroxysmal palpitations, which happens most often with significant physical exertion. If the family has already had cases of early death with such symptoms, then you should consult a doctor in a timely manner.
Diagnostics
Diagnosis is difficult, since the disease is little studied, but, having assessed the totality of all the available signs, it is quite possible to draw the right conclusion. Magnetic resonance imaging, for example, allows you to see the area replaced by connective tissue or fat.
Difficulty in diagnosing the similarity of lesions of the right ventricle like dilated cardiomyopathy and myocarditis. The focal nature of arrhythmogenic cardiomyopathy becomes diffuse only in the last stages. The patient himself, as well as the doctor, should be alerted by frequent fainting. And already during a histological examination, when a biopsy of the wall of the right ventricle is performed, the picture is finally cleared up.
Treatment of arrhythmogenic CMP
Treatment of cardiomyopathy in this case is reduced to a change in lifestyle, a decrease in physical activity, which can somehow slow down the degeneration of the myocardium. Medical treatment is also carried out. These are drugs that prevent arrhythmias. An ICD (cardioverter-defibrillator) is indicated for the high-risk group. In the most severe cases, only a heart transplant saves.
Specific forms of the disease
Ischemic cardiomyopathy
Of all the specific forms of ischemic cardiomyopathy, perhaps the only one that is associated with impaired blood supply to the myocardium. Moreover, the disease manifests itself periodically, to which many patients simply do not pay attention. But if you do not consult a doctor in a timely manner, then it can turn into a severe one. Statistics informs about unfavorable facts: of all patients suffering from a clinical form of coronary heart disease, 58% are patients with ischemic cardiomyopathy. It concerns the disease of middle-aged people, who are observed in the first stages, which leads to a decrease in blood flow.
Alcoholic cardiomyopathy
Alcoholic cardiomyopathy is the most common. The disease is not taken from nowhere, but has a clear causal relationship. Excessive intake of alcohol leads to dysfunction of the cavities of the heart. Initially, slight uneven myocardial hypertrophy is modified, and then continues to progress under the influence of such a poison as ethanol.
As one of the varieties of toxic cardiomyopathy, the alcoholic form can be aggravated by other harmful impurities in alcohol-containing products. And that goes for beer lovers. After all, manufacturers add cobalt to it to increase foaminess, which leads to much more severe poisoning than alcohol.

To begin the treatment of heart disease, you need to limit or eliminate the use of alcohol, as well as restore metabolic (metabolic) processes, which, as a rule, are disturbed in alcoholics. Otherwise, the running process will acquire irreversible forms.
Metabolic cardiomyopathy
I must say that metabolic cardiomyopathy, which at first glance is not much different from alcohol, because it leads to metabolic disorders, has a different nature of occurrence. That is, myocardial dystrophy is caused by other factors, not of inflammatory origin. This may be vitamin deficiency, dysfunction of a particular organ (kidney, liver), excessive exercise. That is, everything that leads to an overstrain of the heart muscle. Alcoholic cardiomyopathy is characterized by inflammation in the heart muscle, and metabolic changes at the cellular level. Although it can also be caused by alcohol poisoning.
The term dysmetabolic cardiomyopathy is also related to heart strain, but against the background of hormonal failure. This often happens at a young age in people who professionally devote themselves to sports. Excessive physical activity against the background of a lack of vitamins and trace elements leads to disruption in the activity of the heart. The causes of metabolic and dysmetabolic cardiomyopathy may have similar causes and symptoms, but the approach to treatment is completely different.
Dishormonal cardiomyopathy
Dishhormonal cardiomyopathy also has a hormonal nature, only among the female population during menopause, when the patient complains of general malaise, pain in the heart, and palpitations. As in the case of the dysmetabolic form, these symptoms do not require cardiac treatment. It is necessary to reduce physical activity, regularly use vitamins. Drug treatment is reduced to mild sedatives like valerian. Rather, psychotherapy and a calm explanation of the doctor about the safety of the symptoms that have overtaken in the menopause play a role in the treatment, since the symptoms are caused by a lack of sex hormones. Sometimes this happens during early puberty, but the symptoms are mild and do not require treatment. However, you should consult a specialist to rule out other, more serious damage to the heart muscle.
So, any slightest change in lifestyle, whether sports loads, puberty or the extinction of the childbearing function, invariably reminds of itself with specific signs that the heart is one of the main organs in the human body.
Video: treatment of hypertrophic cardiomyopathy
Cardiovascular pathologies occupy a leading position among diseases that annually claim millions of human lives. Such gloomy statistics are explained by the fact that the causes of the development of most heart diseases remain unclear.
Cardiomyopathy of the heart is one of the most mysterious diseases, which, although not completely curable, but with adequate therapy, allows a person to live a full life.
Cardiomyopathy cannot be cured, but by catching the disease at an early stage, you can completely control its course, not allowing you to gain the upper hand. To understand when it is necessary to see a doctor, knowing how the heart works, what factors contribute to the development of this pathology, and what symptoms indicate a violation of the function of the heart muscle will help.
Brief information about cardiomyopathy
Cardiomyopathy is a collective name for a group of diseases of the myocardium that disrupt its function. At the same time, any violations, both cardiac and non-cardiac, can have a negative effect on the heart muscle.
In theory, cardiomyopathy can be called any cardiovascular disease. However, most experts tend to attribute some heart ailments to a group of independent diseases.
Since 1995, WHO has adopted a decision on the basis of which the concept of "cardiomyopathy" included any diseases in which the work of the myocardium is disrupted. These include the following common pathologies:
- chronic hypertension;
- cardiac ischemia;
- heart valve defects and others.
However, most experts still do not classify them as cardiomyopathies. Therefore, no one can yet answer which diseases can be attributed to this group. The only pathologies that are not usually combined under these concepts are myocardial dysfunction caused by inflammatory and tumor processes.
The structure and functions of the heart
Cardiomyopathy is a whole group of diseases in which there is a change in the structure and dysfunction of the heart muscle. It is customary to divide the heart into parts, but such a division is conditional.
All parts of the heart are interconnected with each other, therefore, a violation of the functions of one of the parts is reflected in the work of the organ as a whole. To understand the features of cardiomyopathy, one should initially understand how the heart works and what functions each part of it performs.
The heart consists of four chambers:
- the right atrium, where venous blood is collected from the pulmonary circulation;
- the right ventricle, from where blood enters the lungs for oxygenation;
- the left atrium, where arterial blood from the lungs enters after gas exchange;
- the left ventricle, from where blood enters the aorta, and then, through the systemic circulation, delivers oxygen to all organs and tissues.
To prevent arterial and venous blood from mixing with each other during the work of the heart, the left and right chambers of the heart are separated by partitions. The partition between the atria is called atrial, and between the ventricles - interventricular.

Each chamber of the heart has a valve that, when opened, helps blood move from one section to another, as well as enter the lungs and aorta. When closed, the valve prevents backflow of blood.
The wall of the heart consists of three layers, each of which also performs a specific function. These include:
- endocardium - the inner layer, consisting of epithelial cells, which allows unhindered blood circulation;
- myocardium - the middle muscle layer, which, when contracting, pushes blood out of the heart chambers;
- The pericardium is the outer layer of connective tissue.
What factors contribute to the development of cardiomyopathy
Determining the genesis of cardiomyopathy is difficult because many heart diseases can be combined under this concept. In this regard, this pathology was divided into two groups:
- primary, if the cause of cardiomyopathy could not be established;
- secondary or specific, if the cause of its development was any other disease.

Causes of Primary Cardiomyopathy
Among the factors leading to the development of this disease, the most dangerous are the following:
- genetic predisposition;
- viral and bacterial infection;
- autoimmune diseases;
- cardiosclerosis.
Myocardial tissue consists of cardiomyocyte cells that contribute to its contraction. At the same time, cardiomyocytes themselves consist of many protein compounds. In some cases, in the process of intrauterine development of the fetus, a genetic failure occurs, causing a defect in the structure of one of the proteins or several at once, which further negatively affects the work of the myocardium as a whole.
There is an opinion that various viruses and bacteria contribute to the disruption of the myocardium, which tend to penetrate into the cells of the heart muscle and change the structure of the DNA of cardiomyocytes.
In recent years, more and more children with autoimmune diseases have been born. These pathologies are characterized by the fact that the cells of the immune system, instead of protecting, begin to destroy the body's own cells. If they attack the cells of the heart muscle, it will not be possible to cure the disease.

Features of the hypertrophic form of cardiomyopathy
This form of the disease is characterized by thickening of the myocardium in the left ventricle, in which there is a decrease in the volume of the chamber. Since the volume of blood flowing from the left atrium into the left ventricle cannot fit in the reduced space, it remains in the upper chamber. As a result, the walls of the left atrium are stretched and thinned, and blood stasis occurs in the pulmonary circulation.
The thickened layer of muscle mass requires more oxygen, which is not delivered to the heart due to congestion. causes ischemia. In addition, thickening of the myocardium reduces its susceptibility to nerve impulses, as a result of which the contractility of the heart is disturbed.
According to experts, this form of the disease is hereditary. And its development is facilitated by a defect in one of the proteins that make up the structure of cardiomyocytes.
Symptoms of a hypertrophic form of cardiomyopathy
When it occurs, the symptoms mostly remain the same. But to them are added signs indicating a violation of the heart rhythm. The main features include the following:
- causeless fatigue;
- shortness of breath even at rest;
- skin blanching;
- chest pain;
- various perceptual disturbances.

The main danger in this form of the disease is a violation of the heart rate, since this pathology can lead to sudden death.
Features of the restrictive form of cardiomyopathy
In this case, cardiomyocytes are replaced by connective tissue. This feature does not affect the thickness of the muscle layer and does not affect the size of the chambers. However, connective tissue is inelastic and therefore cannot be stretched. As a result, the chambers of the heart are not able to accommodate the volume of blood coming from the systemic and pulmonary circulation, which leads to its stagnation.
Symptoms of restrictive cardiomyopathy
When diagnosing cardiomyopathy, this form helps to identify a small number of manifestations. These include:
- severe shortness of breath, indicating insufficient oxygen supply;
- edema resulting from stagnant processes in both circles of blood circulation.
Classification of secondary cardiomyopathies
Cardiomyopathies that develop against the background of other diseases are divided into the following types:
- toxic (toxic cardiomyopathy most often develops in people suffering from alcoholism);
- ischemic.
Features of dishormonal form of cardiomyopathy
The reason for the development of this form of the disease is a violation of the functions of the endocrine system, leading to an imbalance of hormones. The result of this is a violation of metabolic processes in all organs and tissues, including the myocardium.
The following symptoms may indicate the presence of this form of cardiomyopathy:
- a person has increased nervous excitability even in the absence of obvious reasons;
- there are severe pain behind the sternum and shortness of breath;
- there are fluctuations in blood pressure in the vessels;
- heart rate is disturbed;
- sweating increases.
Features of the toxic form of cardiomyopathy
Toxic cardiomyopathy causes the death of cardiomyocytes and structural changes in the thickness of the muscle layer. It occurs against the background of poisoning with various pharmaceuticals, heavy metals or alcohol.
Among the main manifestations of this type of disease, the following can be noted:
- violation of the pulse rate;
- severe shortness of breath;
- chest pain;
- increased blood pressure;
- swelling of the limbs and face;
- hand tremor.

Other types of cardiomyopathies
There are other types of the disease that do not fall into the general classification, since they combine signs of several forms of the disease at once. A mixed type of cardiomyopathy combines many causes and features that are characteristic of both the primary and secondary forms of the disease.
Diagnosis and treatment
Diagnosis of the disease presents certain difficulties, since doctors are not always able not only to determine the type of cardiomyopathy, but also to distinguish the primary form of the disease from the secondary. Therefore, each patient is assigned a series of diagnostic measures.
- general examination by a cardiologist;
- radiographic examination of the heart.
The treatment regimen for this disease is drawn up after determining its form. The secondary form is easier to treat than the primary, since the manifestations of cardiomyopathy are eliminated after the treatment of the underlying disease that caused structural changes in the myocardium.
In general, for any form of cardiomyopathy, patients are prescribed the following groups of drugs;
- ACE inhibitors;
- increase motor activity, which improves blood circulation, but avoid heavy physical exertion, which increases the need for oxygen in the heart muscle;
- follow a diet that provides for a limited intake of animal proteins, salt and alcohol;
- stop smoking, which increases the risk of developing atherosclerosis;
- be regularly examined by a cardiologist in order to detect any changes in the myocardium in time.
To avoid dangerous consequences, people suffering from cardiomyopathy need to change their lifestyle and diet. To do this, it is recommended to adhere to the following rules:
The pathology under consideration is not fully understood disorders in the structure and functioning of the heart muscle. A couple of decades ago, this pathology was called myocardiopathy, but today this name is not used in official medical sources.
Cardiomyopathy has no age and gender restrictions, and is extremely unfavorable in terms of prognosis.
What kind of disease is cardiomyopathy - the mechanism of occurrence of pathology
In order to understand the essence of this disease, one should begin with an analysis of the term itself:
- « Cardio "(cardio) in Greek means heart.
- "Mio"- everything that is connected with the muscle layer.
- "Pathia" (pathos)- suffering.
Thus, the analysis of this term practically does not clarify the overall picture. Any heart disease provokes painful sensations in the patient.
Video: Cardiomyopathy - general characteristics
The abstraction of the name of the disease in question is due to the fact that today Causes of cardiomyopathy are not well established.. This definition is collective for a number of signs that cause degenerative processes in the heart muscle and ventricles of the heart. All this, ultimately, ends with heart failure or heart rhythm disturbances.
Research reveals violation of metabolic processes in heart cells. Subsequently, this can cause the shrinkage of muscle fibers, as well as the replacement of pathological areas with connective tissue.
Types of cardiomyopathy and causes of the disease - who is at risk?
Depending on the nature of the occurrence of this disease, there are:
- idiopathic or primary cardiomyopathy. What exactly causes cardiac pathology is still not known in this case.
- Secondary. The alleged causes of the development of this cardiomyopathy are:
- hereditary predisposition. A person can inherit a genetic anomaly that causes errors in the structure and function of muscle fibers. The outcome of the disease in hereditary cardiomyopathy cannot be predicted.
- Viruses. This group includes pathogens of influenza, herpes, etc.
- The presence in the anamnesis of information about previous myocarditis.
- Failures in the functioning of the endocrine system. This concerns the detrimental effect of catecholamines and growth hormone on the anatomical structures of the heart muscle.
- The inability of the body's defenses to fully perform their work.
- Harmful effect on the heart muscle of various toxins and allergens. Heavy metals, certain medications, alcohol, and drugs can act as irritants.
In extremely rare cases, the ailment in question is diagnosed in the last months of pregnancy, or in the first half of the postpartum period.
There are 4 main types of this cardiac pathology:
1. Dilated, or congestive
With this form of the disease, myocardial cells in different areas begin to die. The cause of this phenomenon is often inflammatory processes.
The body perceives cells damaged by viral agents as foreign bodies and tries to get rid of them. Once healthy muscle tissue is replaced by connective tissue, which does not differ in plasticity.
In an attempt to cope with its job of pumping blood, the chambers of the heart increase in size. A damaged ventricle of the heart (or both at once) is not able to fully expel blood. This leads to the development of stagnant processes in the ventricles, which is a consequence of the appearance of heart failure.
In addition, the heart works in super mode, trying to provide oxygen to all organs and systems, which leads to the development of arrhythmia.
2. Hypertrophic
It is characterized by thickening and an increase in the mass of the myocardium. As a rule, the left ventricle is involved in the degenerative process, much less often - the right ventricle and septum.
- If pathological changes affect all sections of the heart muscle, they talk about symmetrical cardiomyopathy.
- When the muscle tissue is deformed in the region of the interventricular septum, it is diagnosed asymmetric cardiomyopathy.

With this form of the disease, there is a decrease in the volume of the affected ventricle. Because of this, the blood is not able to fit in the ventricle, and its bulk is concentrated in the atrium, which causes its expansion. Against the background of stagnant processes, oxygen starvation of the myocardium occurs, which negatively affects the pumping function of the heart.
Video: Hypertrophic cardiomyopathy. big heart disease
3. Restrictive
With this type of disease under consideration, the myocardium retains its size and thickness, but its walls lose their elasticity. This leads to an inability to fully pump blood.

Scientists put forward the theory that this form of cardiomyopathy is a complication of other pathologies, but not a separate disease.
The reason for the loss of elasticity of the endocardium is often inflammatory processes. Often, restrictive cardiomyopathy is associated with hormonal disruptions, as well as a violation of lipid metabolism.
4. Arrhythmic
The center of pathological processes in this case is the right ventricle: muscle tissue is replaced by connective or fatty tissue. The left ventricle can also be involved in similar destructive processes.

The danger of arrhythmic cardiomyopathy lies in its consequences: it often leads to the death of the patient.
This disease is extremely rare (1 case out of 5000). However, young people who are actively involved in sports are at risk.
From the information received over the years, it is known that, in some cases, the disease is inherited (although not always). Therefore, people under the age of 40, whose close relatives died at a young age from this disease, should be regularly examined.
In some medical sources, specific forms of this heart disease are classified as a separate group:
- Alcoholic cardiomyopathy. Under the harmful influence of ethanol, which is contained in alcoholic beverages, there is a violation of the functioning of the cavities of the heart, which progresses over time. Beer drinkers are in double danger. Manufacturers add the chemical cobalt to this alcoholic product, due to which a lush foam is formed. But, at its core, cobalt is a poison that provokes more pronounced intoxication than ethanol. In the treatment of alcoholic cardiomyopathy, first of all, alcohol is completely excluded, otherwise the changes will be irreversible.
- Ischemic cardiomyopathy. Associated with disruptions in the blood supply to the heart muscle. The symptomatic picture does not always appear, which is why people rarely seek medical help. However, the lack of adequate therapeutic measures can lead to. At risk are elderly people with initial.
- Metabolic. Associated with failures in the metabolic processes of the myocardium at the cellular level. The reasons for this phenomenon are often intense physical activity, deficiency of vitamins and trace elements, serious errors in the work of the kidneys.
- dishormonal. Most often, they are diagnosed in women experiencing menopause, as well as in adolescents during puberty. Serious damage to the heart muscle in this case does not occur. Therapeutic measures are reduced to minimizing physical activity and taking sedatives.
Video: Cardiomyopathy
The first signs and symptoms of myocardiopathy - how to notice in time?
The symptomatic picture of the pathology under consideration will be determined by its type, as well as the degree of damage to the heart muscle.
With a dilated form, the following negative phenomena are observed:
- Paleness of the skin.
- Swelling of the lower extremities. In advanced stages, fluid accumulates in the lungs and peritoneum.
- Blueness of the face in the region of the nail plate of the fingers.
- Difficulty breathing even with minimal exertion.
- Chest pain that can be relieved by taking nitroglycerin.
- Increase in the diameter of the veins in the neck.
- Increase in blood pressure. Similarly, the body tries to compensate for the lack of oxygen in the blood.
Similar complaints are present in alcoholic cardiomyopathy. Chest pain, however, cannot be relieved with nitroglycerin. Symptoms acquire pronounced features as the number of alcoholic excesses increases. Complaints do not stop within a few days - or a week - after the last drink of alcohol.
It is characterized by similar symptoms as in the previous form of the disease. However, as degenerative phenomena progress, the liver increases in size - it can be felt. Failures in the heartbeat become frequent and pronounced, which often ends in fainting.




