On what day after the operation the skull is returned. Complex operations: consequences of craniotomy. Decompression craniotomy
Cancer and brain tumors video
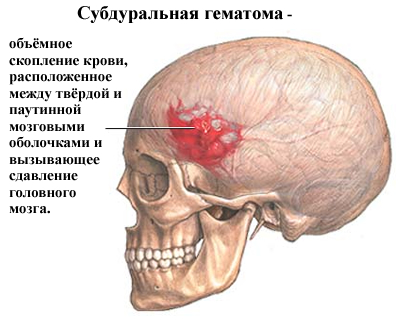
The brain is reliably protected by the bones of the skull, so access to it for both therapeutic and diagnostic purposes is very difficult. The surgical procedure to open the skull is called a craniotomy or craniotomy. The name of this operation "craniotomy" consists of two roots and means that it is associated with the formation of a hole ("tomy") in the skull ("cranio").
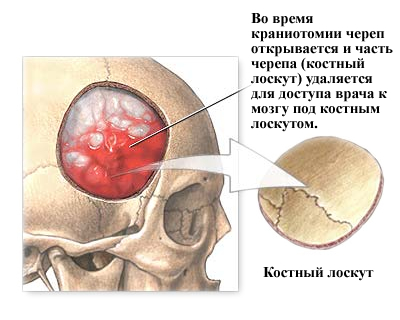
During a craniotomy surgical procedure, the skull is opened and part of the skull (the bone flap) is removed to allow the doctor to access the brain underneath the bone flap. The bone flap is usually replaced after the procedure with tiny plates and screws.
A craniotomy can be small or large, depending on the problem. It can be performed during surgery for various neurological diseases, injuries, or diseases such as brain tumors, hematomas, aneurysms, arteriovenous malformations, or skull fractures. Other causes of craniotomy: extraction of foreign objects (bullets, etc.), cerebral edema, infections. Depending on the reason for a craniotomy, this operation requires a patient stay in the hospital from several days to several weeks.
A craniotomy is any bony opening that is cut into the skull. There are many types of cranial trepanations, which are named according to specific areas of the skull. Usually the bone flap is replaced. If it is not replaced, the procedure is called "removal of skull fragments" or resection.
Craniotomies are also named differently, depending on their size and complexity. The small size is called resection trepanation, or "keyhole", because the bone hole is bitten out with forceps. Sometimes stereotaxic imaging frames or endoscopes are used to direct precise penetration of instruments through these small openings. After resection trepanation, a bone defect remains. If there are indications, the postoperative bone defect is closed with various plastic materials.
Keyhole holes in craniotomy are used for minimally invasive procedures:
Insertion of a shunt into the ventricles to drain cerebrospinal fluid (hydrocephalus)
- insertion of a deep brain stimulator for the treatment of Parkinson's disease;
- insertion of an intracranial pressure monitor (ICP);
- removal of a small sample of abnormal tissue (biopsy);
- Draining of a blood clot (stereotactic hematoma);
- removal of intracranial hematomas;
- to reduce intracranial pressure;
- in the treatment of fractures of the skull bones:
- to install an endoscope when removing small tumors or aneurysms.
Large and complex trepanations of the skull are often referred to as "skull base surgery" or osteoplastic trepanations. These craniotomies involve the removal of the part of the skull that supports the lower part of the brain where the delicate cranial nerves, arteries, and veins are located. Skull base reconstruction is often necessary and may require additional head and neck examination, otology or plastic surgery.
Surgeons often use complex craniotomy patterns. Skull base craniotomy can be used to:
Removal or treatment of large brain tumors, aneurysms, or AVMs;
- treatment of the brain after a skull fracture or trauma (for example, a gunshot wound);
- removal of tumors that affect the bones of the skull.
When is a craniotomy necessary?
The most common indications for craniotomy are:
Benign and malignant brain tumors;
- bleeding (hemorrhage) as a result of a stroke, trauma or blood clots (hematomas) from injuries (subdural and epidural hematomas);
- weakness in the wall of the artery (aneurysm of cerebral vessels);
- damage to the tissues covering the brain;
- foci of infection in the brain (brain abscesses);
- severe nerve or facial pain (eg, trigeminal neuralgia);
- epilepsy
- removal of foreign objects from the head or brain.
Who performs the craniotomy procedure?
A craniotomy is performed by a neurosurgeon, and some physicians have additional training in skull base surgery. A neurosurgeon can work with the head and neck, an otological surgeon with the ear, and an oculoplastic surgeon with the eyes and face.
How to prepare for a craniotomy?
The patient usually has tests (eg, blood work, ECG, chest x-ray) a few days before surgery. In the doctor's office, he signs consent documents and gives full information to the surgeon about his medical history (allergies, medications, reactions to anesthesia, previous surgeries). The patient must stop all non-steroidal anti-inflammatory drugs (Naproxen, Advil, Ibuprofen, etc.) and blood thinners (Coumadin, Aspirin, etc.) 1 week before surgery. It is also necessary to stop smoking any kind of tobacco and alcohol 2 weeks before and 2 weeks after surgery, because all these activities can lead to serious health problems, including bleeding.
How is craniotomy performed?
There are 6 basic steps during a craniotomy. Depending on the underlying problem being treated and the complexity, the procedure can take 3 to 5 hours or more.
Step 1 - patient preparation. No food or drink is allowed after midnight the night before the operation. Craniotomy patients are admitted to the hospital in the morning. General anesthesia is administered intravenously while the patient lies on the operating table. The person falls asleep and their head is in a 3-pin skull fixation device, which is attached to the table and keeps the head upright during the procedure. Inserting a lumbar (spinal) drain into the lower back helps drain cerebrospinal fluid (CSF), which allows the brain to relax during surgery. The patient may be given the brain-relaxing drug Manit.
Step 2 - skin incision. After the scalp is smeared with an antiseptic, a skin incision is made - usually behind the hairline. The surgeon tries to ensure a good cosmetic result after the operation. Sometimes the hair can be gently shaved.
Step 3 - performing a craniotomy, opening the skull. The skin and muscles rise to the bone. Next, the surgeon drills one or more small burrs into the skull with a drill. By inserting a special saw through the burr holes, the surgeon cuts the contour of the bone flap. The cut piece of bone is lifted up and treated with a protective covering of the brain called the "dura mater". The bone flap is securely stored until it is replaced at the end of the procedure.
Step 4 - opening the brain. After opening the dura mater with surgical scissors, the surgeon folds it back to expose the brain. Retractors placed on the brain need to be repaired or removed. Neurosurgeons use special magnifying glasses (loupe, or operating microscope) to see the delicate nerves and blood vessels.
Step 5 is fixing the problem. Due to the fact that the brain is tightly enclosed within the bony skull, the tissues cannot be easily moved to the side, and it is difficult to access them and eliminate all problems. Neurosurgeons use a variety of very small instruments to work deep within the brain. These include long-handled scissors, dissectors, drilling rigs, lasers, ultrasonic aspirators (to break up tumors and suck up debris), computer imaging of guidance systems. In some cases, monitoring is used to stimulate specific cranial nerves while the response is controlled in the brain. This is done in order to preserve the function of the nerves and make sure that they are not damaged later during the operation.

Step 6 - Closing the craniotomy. With the problem of removing or repairing retractors, the dura is also removed from the brain, closed with sutures. The bone flap is placed back in its original position and attached to the skull with titanium plates and screws. Plates and screws are permanently left to support the skull, which can sometimes be felt under the skin. In some cases, drainage tubes may be placed under the skin for several days to remove blood or surgical fluid. The muscles and skin are sutured back together.
The whole procedure lasts 180-240 minutes.
What happens after the operation?
After the operation, the patient is placed in the recovery room, where all his vital signs are monitored as soon as he wakes up from anesthesia. The breathing tube (ventilator) is usually left in place until the patient has fully recovered from anesthesia. Further, he is transferred to the departments of neurology and intensive care for careful observation and monitoring. He will be asked to move his hands, fingers and toes, and feet frequently.
The length of stay in the hospital ranges from 2-3 days to 2 weeks - depending on the complexity of the operation and the development of any complications. When the patient is released from the hospital, he will be given a series of instructions. Stitches or staples are removed 7-10 days after surgery in the doctor's office.
Recovery after craniotomy
Craniotomy is a complex surgical intervention with a relatively long recovery period. Here are some tips that can alleviate the patient's condition after craniotomy:
- Discomfort. After surgery, the headache is managed with narcotic drugs. Since narcotic pills are addictive, they are used for a limited period (no more than 2-4 weeks). Their regular use can also cause constipation, so while consuming them, you need to drink plenty of water and eat foods high in fiber. Laxatives (eg, Dulcolax, Senocott, Senadexin, Milk of Magnesia) can be purchased without a prescription. Thereafter, pain is managed with acetaminophen (eg, Tylenol) and NSAIDs (eg, Aspirin, Ibuprofen, Advil, Motrin, Nuprin, Naproxen, Aliv).
An anticonvulsant may be temporarily prescribed to prevent seizures. Anticonvulsants common to all: Dilantin (Phenytoin), Tegretol (Carbamazepine) and Neurontin (Gabapentin). Some patients develop side effects caused by these anticonvulsants (eg, drowsiness, balance problems, rash). In such cases, blood samples are taken to monitor drug levels and manage side effects.
- Restrictions. After a craniotomy, you should not drive until your surgeon tells you to, for an extended period of time. Also, do not lift heavy loads (eg a 2 liter bottle of water), including children.
In the first weeks after the operation, heavy work around the house and in the office is not allowed. This includes: gardening, mowing, vacuuming, ironing and loading/unloading the dishwasher, washing machine or dryer.
Under no circumstances should alcoholic beverages be consumed.
- Activity. Gradually, you need to return to your normal activities. Fatigue is common.
Early Exercise Program - Gently stretching the neck and back may be recommended. Walks are recommended. You need to start with short walks and gradually increase the distance. Do not engage in other forms of exercise without permission from your surgeon.
- Bathing. The patient can shower with shampoo 3-4 days after the operation. Stitches or staples that remain in place when the patient is discharged should be removed 7 to 14 days after surgery. The patient should ask their surgeon or call the office when this can be done.
- Recovery. The recovery time varies from 1 to 4 weeks - depending on the underlying disease being treated and the overall health. Full recovery can take up to 8 weeks. Walking is a good way to increase your activity level. You need to start with short, frequent walks in the house and gradually try to go outside. It is important not to overdo it, especially if the person is continuing treatment with radiation or chemotherapy. The surgeon can tell his patient when he can gradually return to work.
Risks and complications of craniotomy (craniotomy)
Any surgical intervention is not without risk. Common complications from any surgery include: bleeding, infection, blood clots, reactions to anesthesia. There may be specific complications associated with craniotomy: convulsions; swelling of the brain, which may require a second craniotomy; nerve damage, which can lead to muscle paralysis or weakness leaks that may require repair; loss of mental functions; irreversible brain damage with associated disabilities, etc.
Forecast of craniotomy (craniotomy)
The results of a craniotomy depend on the underlying condition being treated..
Before considering the consequences of trepanation of the skull, I would like to define this term, since not everyone has an idea of what will be discussed. So, trepanation is an operation in which a hole is made in the skull bone in order to have access to the underlying cavity, as well as to intracranial formations in order to eliminate them. It is believed that this surgical intervention is designed to help patients, as it is carried out only in case of emergency. But we must also remember that this is also a kind of trauma that has its consequences.
Trepanation: what determines its result
The consequences are quite strongly dependent on the size, degree and severity of brain damage before surgery. And the deeper and more extensive the surgical intervention, the greater the risks and negative results of its implementation. In addition, the accuracy of the operation and the qualifications of the specialist who conducts it play an important role.
Disability or death?
It should be noted that a patient who has gone through a trepanation is given a disability, which can be canceled if the human body is fully restored over several years. But also surgical intervention can cause disastrous consequences, since trepanation sometimes leads to death, so it is very difficult to predict.
Postoperative period

After the operation, a rubber tube with holes is inserted under the bone flap, through which blood accumulated in the wound will flow through the seams. If the meninges are not tightly sewn up, such blood can flow out along with the cerebrospinal fluid. This can lead to the most dangerous complications, such as liquorrhea. The contents of the skull can become infected, often leading to encephalitis and meningitis. To prevent this from happening, additional sutures are placed at the wound site.
The outcome of trepanation
Some of the effects of a craniotomy are similar in many people. In the postoperative period, most patients experience swelling of the soft tissues of the eyelids and forehead, as well as bruising in the eye area due to the formation of a hematoma inside the skull. Almost always, patients complain of headaches, increased pressure, vomiting and nausea.
Occurrence of defects
Many who have undergone such a surgical operation (especially for children and young people) are faced with such a problem as deformation of the skull area and the formation of dents. These defects do not disappear with time and require plastic surgery to prevent post-trepanation syndrome.
Rehabilitation process

Rehabilitation after craniotomy at first should take place at home. At the same time, it is forbidden to play sports (you can not tilt your head down). Lifestyle should be sedentary. The place of trepanation must remain clean, blood must not be allowed to freeze, as this can lead to the formation of blood clots and hematomas, as well as an increase in
Conclusion
Thus, the consequences of craniotomy can be completely different, and most importantly, unpredictable. Therefore, such a surgical operation is always risky and is performed only in case of emergency.
Craniotomy is a surgical manipulation that can be performed in a hospital of any level as an emergency medical care for patients with intracranial hypertension.
Craniotomy has been known since ancient times. Even ancient people with the help of trepanation treated almost all diseases, believing that the evil spirit of the disease leaves through the hole in the skull. Now this medical manipulation is carried out exclusively for health reasons or in order to improve the prognosis of a brain disease.
Operation technique
During trepanation of the skull, the cranium is opened - the bones of the skull. This is needed for two purposes:
- Remove intracranial hypertension (edematous fluid or blood will flow through an artificial hole, which will prevent a life-threatening complication - wedging of the brain).
- Perform medical manipulations on a living brain. For example, removing a brain tumor.
The opening of the bones is performed using special tools. If you just need to relieve hypertension, usually make one small hole in the parietal bone with a milling cutter. This is less traumatic, and therefore more favorable in terms of rehabilitation and health consequences. If wide access to the brain is needed, an extensive trepanation is performed with the removal of part of the bone.

Types of craniotomy
Before talking about the methods of craniotomy, you need to consider the structure of the bones of the skull. The bones of the cranial vault are represented by plates, from above they are covered with periosteum, and from below they are adjacent to the dura mater. The periosteum is the main nourishing tissue of the bones. The main supply vessels pass through it. Damage to the periosteum leads to bone death and necrosis.
Based on this, the opening of the cranium can occur in five ways:
- Osteoplastic trepanation. This is a classic method of opening the cranium. During it, a section of the parietal bone is cut out without damaging the periosteum. The periosteum connects the sawn part of the bone with the rest of the cranial vault. Due to the preservation of the periosteum, the nutrition of the bone during the operation does not stop; after the end of the medical manipulation, the bone is placed back in its place with the periosteum sutured. Thus, the operation on the brain takes place without a defect in the bones of the skull, which has the best prognosis for rehabilitation and recovery.
- Resection type of trepanation - has less favorable health consequences and a less favorable prognosis for rehabilitation after surgery. With this type of trepanation, the sawn section of the parietal bone is removed along with the periosteum; its restoration in the future is impossible. The defect is covered by soft tissues (dura mater and skin with the scalp), which has a less favorable prognosis and a high risk of complications.
- Trepanation for the purpose of decompression. The main task of the doctor is to create a hole in the bones of the skull without further expansion of the defect. Through the hole formed, the agent that caused intracranial hypertension is eliminated: blood, cerebrospinal fluid, edematous fluid or pus are removed. Such an operation does not require special rehabilitation, the negative consequences for health are minimal.
- In neurosurgery operating rooms, awake craniotomies can be performed. They are performed without turning off the patient's brain. This is necessary in cases where the pathological area is located close to the reflexogenic zones. In order not to damage these structures during the manipulation, the patient’s consciousness is not turned off, but they constantly look at his reaction, the activity of the organ and correlate all this with the actions of the surgeon. Such an intervention is favorable in terms of prognosis and health consequences, but rehabilitation after it is no less difficult for the patient.
- The latest word in medicine in the field of neurosurgery is stereotaxy. The doctor uses a computer to access pathological tissues. This reduces the risk of touching and damaging healthy tissues, the computer accurately calculates the pathological area, after which the surgeon removes it. This is favorable in terms of predicting health consequences; rehabilitation in such patients occurs without complications.

Preparing for the operation
The manipulation does not require special preparation. If trepanation is performed in a planned manner, immediately before the operation, the patient washes his head thoroughly and does not eat. Directly on the operating table, a section of hair is shaved, where trepanation incisions will be made, and this is where the patient's preparation ends.
The type of anesthesia is chosen by the surgeon depending on the type of trepanation performed. Most often, general anesthesia is used, which subsequently turns off the brain and all types of sensitivity. With stereotaxy, local anesthesia is predominantly performed. And when it is necessary for the patient to be conscious, anesthesia is not performed at all or the skin at the incision site is anesthetized.

Postoperative period
Rehabilitation and prognosis on the first day after surgery
The first day the patient is in the intensive care unit, unconscious. The functions of vital systems are provided by the ventilator and parenteral nutrition. At this time, it is important to monitor the patient's condition, as there is a risk of missing the onset of a formidable complication. In terms of rehabilitation, it is important to provide complete not only physical, but also emotional peace to the patient. The prognosis on the first day is doubtful, since it is impossible to predict the reaction of the brain to this type of intervention.
Rehabilitation and prognosis in the first week after surgery
After stabilization of the condition, the patient is transferred to the general ward of the neurosurgery department. This period is less dangerous in terms of complications, the prognosis for rehabilitation and restoration of health is more favorable, but the consequences are still impossible to predict. The brain begins to activate, perform its usual functions, and establishes new neural connections. Here it is important to properly care for the operated:
- To improve the outflow of fluid from the brain, the patient's head should always be in an elevated position. If the head end of the bed does not rise, place a few pillows under your head, just enough to make it comfortable. The patient should also sleep in a semi-sitting position.
- Do not give the patient a lot of drinking water and other drinks. To relieve intracranial hypertension, you need to remove fluid from the body. It is allowed to drink up to 1 liter of liquid per day.
- Rehabilitation for intracranial hypertension is dangerous due to the occurrence of indomitable vomiting, so stock up on antiemetic drugs.
- Ensure that the patient takes all prescribed medications on time. Antibiotics are usually prescribed to prevent infection. Timely intake of drugs improves the prognosis of the disease, contributes to the speedy rehabilitation and reduces the risk of negative consequences.
- Keep the postoperative wound clean, change dressings regularly. This will reduce the risk of infectious consequences that are dangerous to health.
- Activate the patient as early as possible. On the second day of transfer to the regular ward, begin to help the patient walk around the ward. The risk of postoperative pneumonia will decrease, blood circulation and the prognosis as a whole will improve.
- Watch the patient's diet, especially on the first day after trepanation. Food should be highly fortified, contain a large amount of proteins and nutrients. After discharge, the patient can eat their favorite foods, but also try to enrich the diet with vitamins, which are so necessary for brain function.

Rehabilitation and prognosis after discharge
With an uncomplicated course of the recovery period, the prognosis for operated patients is favorable. After discharge from the hospital, limit physical activity. It is not allowed to perform exercises with head tilts to the side, forward and down. To restore brain function, increase the number of leisurely walks up to 1 hour a day, if possible more. Take the drugs prescribed by your doctor, review your diet and add more vitamins and nutrients to it.
Important! At home, constantly monitor the condition of the postoperative scar to prevent local and generalized infectious consequences. To do this, treat it daily with an antiseptic solution (alcohol tincture of iodine, brilliant green (brilliant green), potassium permanganate solution). Do not wet the scar for a month. If you suspect inflammation or suppuration, contact your doctor immediately.
Important video: Technique of surgical trepanation of the skull
Consequences after trepanation and complications
The human brain is an organ whose function is impossible to predict. After trepanation, the consequences for each person are individual, since the work of the central nervous system is different for everyone. The variety of consequences and complications after trepanation makes surgeons monitor patients for life, especially during the rehabilitation period. That is why no qualified doctor can give you an accurate forecast.
Among the consequences are:
- Infectious consequences that worsen the prognosis and rehabilitation: meningitis, meningoencephalitis, suppuration of the surgical wound, sepsis and septic shock.
- Violations of the work of analyzers: visual, auditory, olfactory.
- Epileptic seizures, up to status epilepticus. Paralysis, convulsive seizures.
- Changes in cognitive functions: memory, speech, attention, thinking.
- Edema of the brain.
- Bleeding.
- Thrombosis of the veins of the brain and, as a result, a stroke.
We should not forget one more cosmetic consequence: the deformation of the skull. After resection trepanation, the shape of the patient's skull changes due to the fact that part of the bone is removed. At the site of the defect, an impression in the patient's skull will be visible.
Craniotomy in medical circles is a rather complicated operation, known to the ancient Aesculapius, when doctors treated tumors, internal hemorrhages and injuries by opening the skull.
At its core, trepanation is the creation of a hole in the skull bone and the opening of access to the gray matter of the brain, blood vessels and its membrane, pathological neoplasms. It has its own strict indications for carrying out, but in the state of shock and thermal condition of the patient, as well as in other cases, it has certain limitations for carrying out.
Medical indications for trepanation
Modern medicine is developing every year and the indications for trepanation are becoming less and less - this is achieved through the use of less traumatic methods and methods of treatment. But today it is trepanation that is the only method in certain situations to quickly cope with the pathological process, preventing the development of irreversible, negative consequences.
Doctors note that the reasons for conducting a decompressive type of trepanation are diseases that contribute to a sharp increase in intracranial pressure, a shift in the gray matter of the brain relative to its normal position. This threatens with subsequent infringement and a high risk of death. In this case, we are talking about such pathological changes:
- intracranial types of cerebral hemorrhage;
- head injuries, bruises, combined with the formation of edema and hematomas;
- brain abscess and large in size, inoperable types of neoplasms;
With the help of this type of trepanation, the pathology is not eliminated, but its consequences that are dangerous for the patient are eliminated.
The process of preparing for surgery
If it becomes necessary to apply a craniotomy, the preliminary preparation of the patient for surgical intervention is of no small importance. If there is enough time and surgery is carried out as planned, the doctor prescribes a comprehensive examination. In this case, the doctor prescribes the delivery of laboratory tests, an examination using MRI and CT, as well as an examination and consultation of highly specialized medical specialists. Obligatory examination and consultation of the therapist - he decides the need for trepanation.
If there is no time and the surgical intervention is carried out in a short time and the surgeons have little time for preparation, the patient undergoes a minimum of examinations. In particular, this is a general and biochemical laboratory blood test, MRI or CT - they will help to accurately determine the location of the pathology, coagulogram.
If the surgical intervention is planned, then on the eve of the operation, after 6 pm, the patient is forbidden to drink and eat, he is examined and consulted by a surgeon and an anesthesiologist. The main thing at this stage is to concentrate, relax and not worry, and if nervousness is increased, then take sedatives. Before the operation on the head itself, the hair is shaved, the area is treated with anesthetics, and the skull is fixed in the position necessary for the surgeon and the full operation. The patient is put to sleep under anesthesia and the work of the surgeon begins.
Trepanation methods
In the practice of surgeons, trepanation is performed by one of the methods described below.
- Osteoplastic type of trepanation. In this case, the doctor opens the skull in the area where the path to the affected area of the brain is the shortest. First of all, markings in the form of a horseshoe on the skin are sequentially made, then the soft tissues on the head are separated - in this case, the skin flap is at the bottom, thereby preventing a malfunction in the blood flow. For the most part, the width of the separated skin area on the head does not exceed 6-7 cm, then the doctor drills through the cranial bone, gets to the dura mater, and, dissecting it, penetrates into the cranial cavity. After that, all the necessary surgical procedures are carried out -
- Resection type of trepanation - it is carried out when diagnosing an intracranial tumor, which cannot be removed due to rapid cerebral edema due to injuries and hematomas. Most often, it is carried out in the temporal region, since the bones of the skull protect the temporal type of muscles, and it is she who will block the trepanation window, reliably protecting in the future. With regard to the cosmetic effect, the stitches are less visible behind the ear and the patient does not suffer from external discomfort as much.

Osteoplastic trepanation of the skull in the fronto-parietal-temporal region.
At the beginning of the surgical intervention, the doctor removes a horseshoe-shaped flap of skin and muscles, turns it away, then cuts the periosteal tissue. He makes a hole in the bone with a cutter - as a result, a hole is obtained in the form of a trapezoid in diameter from 5 to 10 cm. During intracranial decompression, the doctor gradually removes the dura mater and performs the necessary decompression manipulations. The completion of the surgeon's work is the suturing of tissues - in this case, the hard shell of the brain is not affected. The doctor does not lay the bone area on it - if there is an external defect, then it can be eliminated with the help of synthetic medical materials.
Postoperative period and patient recovery
After the operation, doctors monitor the patient's condition around the clock, monitoring the work of his internal organs and systems. Most often, on the 2-3rd day, the patient can be transferred to the neurosurgery department if the operation is successful and spends about 2 weeks there.
During the entire period of the patient's stay in the hospital, it is important to monitor the waste of excess fluid through the drainage system, the condition of the hole during the resection type of trepanation. If the patient is diagnosed with swelling of the face and dark circles under the eyes, swelling at the site of the surgical intervention of the bandage, most likely, postoperative hematoma and cerebral edema develop.
As an operative intervention, trepanation is always accompanied by a high risk of various complications - infections and inflammations, meningitis and encephalitis, hematomas with insufficient hemostasis and failure of the sutures themselves. The negative consequences of opening the skull can be:
- neurological nature of the disorder due to damage to the lining of the brain, blood vessels and tissues;
- defeat and disorder of motor activity and decrease in sensitivity;
- intellectual disorders and convulsions;
According to doctors, the most dangerous negative consequence after a craniotomy is the leakage of cerebrospinal fluid from wounds. This can provoke infection and the development of meningococcal encephalitis.
No less serious, cosmetic defect is a violation of the symmetry of the skull, its deformation - in this case, doctors carry out methods of cosmetic surgery and correction. To protect the brain tissue, gray matter - after a resection type of trepanation, doctors close the wound with synthetic, special plates.
The course of rehabilitation and recovery after opening the cranium provides not only drug therapy, but also the elimination of the neurological type of disorders, as well as the patient's adaptation, both in work and in society. While the doctors have not removed the stitches, the wound is treated daily, the dressings are changed, but the patient can wash his head and hair only after 2 weeks after the intervention of the surgeons.
If the patient is worried about bouts of severe pain, the doctor prescribes analgesics, with a negative manifestation of seizures, anticonvulsants. Doctors compose the entire course of recovery and rehabilitation taking into account the nature of the pathology, which became the basis for trepanation.
After surgery, the patient can undergo a rehabilitation course and learn to walk and talk again, gradually restoring memory and other functions impaired by the pathology. Not only bed rest is shown, but also the exclusion of emotional, psychological and physical stress. In case of serious and severe disorders of speech and memory, thinking, the patient is shown additional care, a specialized rehabilitation course, taking into account the negative consequences. In some cases, disability is established - this issue is decided by a special medical commission, taking into account the patient's condition, the degree of damage and negative consequences.
In order to understand what craniotomy is and what risks the procedure contains, one should understand in detail the intricacies of the operation and the most characteristic consequences that arise after its implementation. Trepanation, or opening of the cranium, is an osteoplastic procedure that is performed to eliminate pathological structures in the brain area. Such formations include hematomas, head injuries, critical conditions that call into question the life of the patient, for example, or the consequences of increased intracranial pressure and blockage of blood vessels.
The operation is aimed at correcting a wide range of pathological conditions associated with a violation of the structure of the brain. Despite the high risks of the procedure, in some cases the nature of the damage leaves the only chance for human survival.
Indications for the procedure
Doctors prescribe trepanation to eliminate various disorders in the brain area. The operation is carried out with:
- the presence of oncological structures in the brain area;
- damage to blood vessels;
- therapy of nervous disorders;
- pressure inside the skull;
- the presence of tissues infected with pathogenic microorganisms;
- pathology of blood vessels in the area of hard tissues of the brain;
- abscesses and damage to brain structures;
- head injuries, fractures;
Surgery is sometimes necessary to take tissue samples for biopsy. What a craniotomy is done for is determined in each case by the doctor's testimony. Among the tasks of the procedure are:
- elimination of pathological tissues detected during the diagnosis of neoplasms, the growth of which threatens to damage parts of the brain;
- removal of excess pressure inside the skull if it is impossible to perform an operation in the presence of a tumor;
- elimination of hematomas of various sizes, localization of the consequences of hemorrhage in stroke;
- restoration of the integrity of the cranium after acquired or birth injuries.
It should be noted that a certain percentage of the procedures when a craniotomy is performed is not carried out in order to eliminate the violation at a late stage of the disease, but to eliminate possible complications associated with the development of pathology.
The essence and types of the operation
Trepanation is performed after a preliminary diagnosis using the following methods:
- angiography;
- duplex study of blood vessels using ultrasound;
- conducting a study of the area using devices.
Such studies are necessary to determine the type of disorder and the area of localization of the pathology, assess the degree of damage to structures, and make a prognosis of the probable course of the disease. The data obtained is used to select the method by which a craniotomy is performed after an injury, and also help to predict what consequences may occur after the operation.
The procedure can be performed in a planned manner, for example, in the case of removal of tumors, or be of an emergency nature, associated with the elimination of the consequences of a cerebral hemorrhage. The operation itself is performed in specialized inpatient departments of neurosurgical clinics with the involvement of highly qualified surgeons, whose priority is to save human life.
The way a craniotomy is done involves drilling a hole at the location of the pathology or cutting out part of the bone structure, carried out after using general anesthesia and removing the skin from the site of the procedure.
Then the cut out section is removed and the hard shell is removed. After that, an operation is performed directly to eliminate the pathology inside the skull, followed by the return of the bone area to its place and fastening with titanium plates, screws or by performing osteoplasty. Specialists distinguish between such types of procedures as:
- An osteoplastic procedure, for which an oval-shaped or horseshoe-shaped incision is made, is performed at the base of the skull at an angle to prevent the cut part from falling into the box. After that, the cut out area is eliminated, and the procedure is carried out according to the mechanism described above. If it is necessary to divert blood or fluid accumulated in the area of pathology, a drainage tube is mounted in the area of intervention, followed by bandaging of the head.
- Craniotomy or craniectomy is performed while the patient is conscious and involves the use of sedatives and local anesthesia of the area where the procedure is performed to suppress the patient's sense of fear. The expediency of such an operation is that the doctor receives feedback that excludes damage to vital connections in the patient's brain.
- Stereotaxy involves the use of computer technology to examine certain areas of the brain before trepanation. In this case, the operation is performed in a non-invasive way, by applying a gamma knife through a special helmet worn on the patient's head. The device operates on the principle of precise treatment of areas with pathological tissues with directed beams of radioactive cobalt. The disadvantages of the method include the possibility of destruction of formations no larger than 35 mm.
- The resection type of intervention involves making a hole of small diameter with its expansion as necessary to the desired size. Unlike the classical method of trepanation, the brain in this type of procedure is not covered with bone tissue after it is completed. The protective function in this method is assigned to the soft tissues and the dermis layer covering the site of the intervention.
- Decompression trepanation is performed to reduce the value of intracranial pressure. If the location of the pathology is known, a decompression incision is made above it, otherwise the incision is made in the form of a downward-facing horseshoe in the temporal region from the side.
Considering the severity of pathologies that are indications for craniotomy, violation of the integrity of bone structures, high probability of traumatism of blood vessels and nerve cells, the possibility of consequences after the operation is of high importance, regardless of the severity of the disease.
Recovery after trepanation
The recovery period after the procedure is no less important than the procedure itself. The procedure after trepanation is reduced to the following measures:
- The presence of the patient during the day after the operation in the intensive care unit under the supervision of qualified specialists using devices for monitoring and maintaining the patient's condition. After that, the sterile dressing is removed from the wound, and the area where the intervention was performed is subjected to constant antibacterial treatment.
- Recovery in the hospital for the next week with a possible increase in the time spent under the supervision of specialists in case of complications associated with trepanation. After a few days, if there are no contraindications, the patient is allowed to get up and walk short distances. Experts recommend starting walking as soon as possible, as this measure will prevent the occurrence of pneumonia and the formation of blood clots.
- In the process of care, it is necessary to ensure an elevated position of the patient's head, which is necessary to reduce blood pressure. Patients are restricted from fluid intake.
- The drug course may include taking anti-inflammatory, anticonvulsant, antiemetic, sedative, analgesic and steroid drugs.
Rehabilitation after trepanation of the skull, carried out after discharge (7-14 days) at home, includes:
- Limiting the severity of lifted loads and doing sports or yoga, excluding actions associated with head tilts.
- Elimination of exposure to moisture on the area of intervention for a long time. If there is a change in the color of the postoperative scar or other abnormalities that occur during the healing process, you should immediately consult a doctor.
- Taking the recommended medications and folk remedies agreed with the doctor, which help to speed up the rehabilitation process.
- Compliance with the recommended diet.
- Despite the restriction of sports, doctors recommend that the patient take walks under the supervision of relatives and perform simple physical activity, the weight of the lifted loads should not exceed 3 kg.
- The success of the operation and the duration of rehabilitation largely depend on the patient's bad habits. Smoking and strong emotional outbursts increase the risk of an unfavorable outcome, therefore, in the postoperative period, it is necessary to abandon them.
- If necessary, you may need to take a course of classes with a speech therapist to restore speech function.
The listed rehabilitation measures provide for the normal course of the recovery process, the duration of which may exceed 3 months. However, it should be noted that no one gives guarantees during the operation, its result can be both a significant relief of the patient's condition, and a relative improvement against the background of complications resulting from the intervention.
Complications after trepanation
The risk of an unsuccessful outcome when performing neurosurgical procedures to eliminate pathologies in the cranial region is difficult to overestimate. Some people as a result of this are deprived of their usual way of life, forced to change jobs due to the emergence of health restrictions. Such patients are often interested in the attending physician whether they give a group after a craniotomy. This question can only be answered by evaluating the results of the intervention.
Disability after the procedure is given for a period of three years upon detection of a condition that limits the full life of the patient. The disability group is assigned by a qualified council of specialists, evaluating the results of the examination for the detection of pathological abnormalities in the work of vital functions. With the improvement of the patient's condition during the subsequent recommission, the disability group is canceled.
Among the most common consequences associated with the procedure, patients name:
- the appearance of bleeding;
- increased body temperature;
- pathology of the organs of vision and hearing;
- memory impairment;
- dysfunction of the urinary and digestive systems;
- the appearance of infections in the intestines, bladder and lungs;
- swelling;
- fever;
- frequent, severe headaches;
- mismatch of the movement coordination system;
- nausea and vomiting;
- decreased sensitivity and numbness of the organs of perception, as well as limbs.
- difficulty breathing and shortness of breath;
- chills;
- violation of speech function;
- the appearance of asthenic symptoms;
- fainting;
- convulsions and paralysis of the limbs;
- coma state.
In order to avoid the occurrence of complications, the patient must maintain constant communication with the attending physician, reporting any violations in the postoperative period.
Treatment of complications
For the timely detection of violations of the behavior or consciousness of the patient, weekly consultations with the attending physician are recommended. During the rehabilitation period, it is possible to prescribe a course of massage or physiotherapy to the patient, visit a psychologist and a neuropathologist. Depending on the type of complications that occur, the doctor may recommend treatment:
- If inflammation of the bladder, intestines and lungs occurs, antibiotics are used. The appearance of infections during this period is associated with a weakening of the body's immune system and restrictions on the patient's movements. Therefore, the prevention of pathology is the implementation of exercises from the exercise therapy complex, compliance with the sleep regimen and the prescribed diet.
- The formation of blood clots associated with immobility carries the risk of blockage of blood vessels. Depending on the organ in which it occurs, the possible consequences are manifested: heart attack, stroke, paralysis. In severe cases, complications for the patient can result in death. As measures to prevent the development of events in a similar scenario, the patient is recommended to take drugs that help thin the blood and take daily walks.
- Violations of the neurological type, which are permanent or temporary, appear due to swelling of the tissues surrounding the structure of the brain. To minimize the consequences of such disorders, it is recommended to take anti-inflammatory drugs.
- Bleeding that occurs after the procedure, in most cases, continues for several days. In the case of localization of blood in the area of nerve processes or motor centers in the skull, they cause seizures. In rare cases, with bleeding that is profuse, repeated trepanation is recommended. In most situations, such a pathology is eliminated by drainage, which ensures the removal of blood.
When asked by patients how long they live after craniotomy, it is difficult to give any exact answer, since with the successful completion of the procedure, a direct relationship between the fact of the procedure and a reduction in life expectancy was not found. On the other hand, with a negative outcome of the operation, life expectancy may be reduced.



